HIV Risk Calculator & Complete Exposure Guide (2026)
🕓 Last updated: 03 May 2026
A private HIV risk calculator that turns exposure details into a clear, evidence-informed risk estimate.
HIVRiskReport is a private, educational tool that estimates the statistical risk of HIV transmission from a single sexual encounter. It uses published epidemiological data from sources such as the CDC and peer-reviewed medical studies to translate multiple risk factors into one clear probability, shown as both a percentage and a “1 in X” figure. This report does not diagnose HIV or predict individual outcomes, but it helps replace vague anxiety with realistic context and guidance on appropriate next steps, including testing when needed.
CALCULATE YOUR HIV RISK USING OUR
PROPRIETARY, PRIVATE
AI ASSESSMENT TOOL.
Built to replace vague panic with structured probability, testing guidance, and clear next steps.
Table of Contents
Use this guide to understand HIV exposure risk, testing windows, PEP, PrEP, condoms, transmission routes, and the factors used in a personalized HIV risk calculation.
Your clear, structured path through HIV risk
This guide was created to help you understand HIV transmission risk using real data, clear logic, and step-by-step explanations. No guesswork, no conflicting articles, and no panic loops, just a grounded framework you can follow from start to finish.
This section groups common HIV anxiety scenarios into symptoms, exposure types, testing questions, and prevention topics so you can find the most relevant guide quickly.
Most Common Scenarios Explained
Symptoms people commonly panic about
These guides explain why symptoms alone cannot diagnose HIV, what common lookalikes exist, and when testing is the right next step.
Panicking over a rash after sex? This guide explains what an acute HIV rash can look like, how it differs from common skin issues, and why timing plus proper testing beats symptom-scanning.
Read More →A sore throat can trigger major anxiety. This guide breaks down the difference between acute HIV symptom fear and more common explanations like allergies, colds, reflux, irritation, or ordinary viral illness.
Read More →Worried that oral thrush, white tongue, or tongue changes could mean HIV? This guide explains common non-HIV causes, what HIV-related mouth findings can look like, and when testing matters most.
Read More →Swollen glands can happen for many reasons. This guide explains when HIV-related lymph node swelling can occur, what patterns matter, and why testing matters more than checking your neck repeatedly.
Read More →Worried that brittle nails, ridges, colour changes, or brown nails could mean HIV? This guide explains what HIV can and cannot do to nails, and what is more commonly causing nail changes.
Read More →It is easy to worry about symptoms after a possible exposure. This guide helps separate unreliable signs from useful information, so you can focus on testing instead of fear.
Read More →Sex act and exposure risk guides
These pages explain how risk changes by sex act, partner context, condom use, and biological route of exposure.
Anal sex can trigger major HIV anxiety, but the real risk depends on role, viral load, and prevention. This guide breaks down receptive vs insertive risk, condoms, PrEP, U=U, PEP, and testing.
Read More →This common question deserves a clear answer. This article breaks down the real risk of HIV from oral sex, separating myths from medical facts.
Read More →Worried about HIV after sex with a condom? This guide explains whether HIV can pass through an intact condom, what condom failure really means, and how to think clearly after protected sex.
Read More →What is the real connection between sex work and HIV risk? This article looks past stigma and explains the facts, context, and factors that matter most.
Read More →HIV transmission from female to male is statistically less efficient than some other routes. This article explains the biological reasons and what still matters.
Read More →Curious whether circumcision makes sex safer? This article explains how circumcision changes risk for insertive partners and why viral load, condoms, and PrEP still matter more.
Read More →Pre-cum is not semen, but it can carry HIV under specific conditions. This article explains how viral load, urethral shedding, mucosal tissue, and U=U affect real-world risk.
Read More →Worried about HIV in the air, on surfaces, or in dried fluids? This guide explains what actually happens to HIV outside the body and why everyday contact is not a realistic route.
Read More →Testing, PEP, PrEP, and prevention
These guides help you understand what to do after a possible exposure, including prevention choices and testing windows.
Feeling worried about prevention? This guide explains the difference between PrEP before exposure and PEP after exposure so you can understand your options clearly.
Read More →Worried after an HIV exposure? This article explains when PEP is usually recommended, when doctors assess it case by case, and when it is usually not recommended.
Read More →Wondering what undetectable actually means for HIV transmission? This article explains viral load, U=U, and how effective treatment changes sexual transmission risk.
Read More →Timing is key for an accurate HIV test result. This guide explains the window periods for lab blood tests and at-home oral tests so you can choose the right one.
Read More →Learn how oral HIV tests like OraQuick work, what triggers the test and control lines, and why properly timed results are generally trustworthy.
Read More →Anxiety, behaviour, and the calculator itself
These pages explain why HIV anxiety can spiral and how a structured risk calculation can help you move from fear to a plan.
Feeling anxious after a possible exposure is normal. A risk calculator can help you look past fear and see your situation through facts, probability, and testing logic.
Read More →Feeling stuck in a cycle you can’t control? This guide breaks down compulsive sexual behaviour, explains the habit loop, and gives a practical recovery plan.
Read More →HIV Testing Timeline Calculator
Knowing when you can test and trust the result is often just as important as knowing the probability itself. This section gives general windows, however your personalized report uses your actual encounter date to generate exact earliest and conclusive test dates, based on the best available evidence from organisations such as CDC.
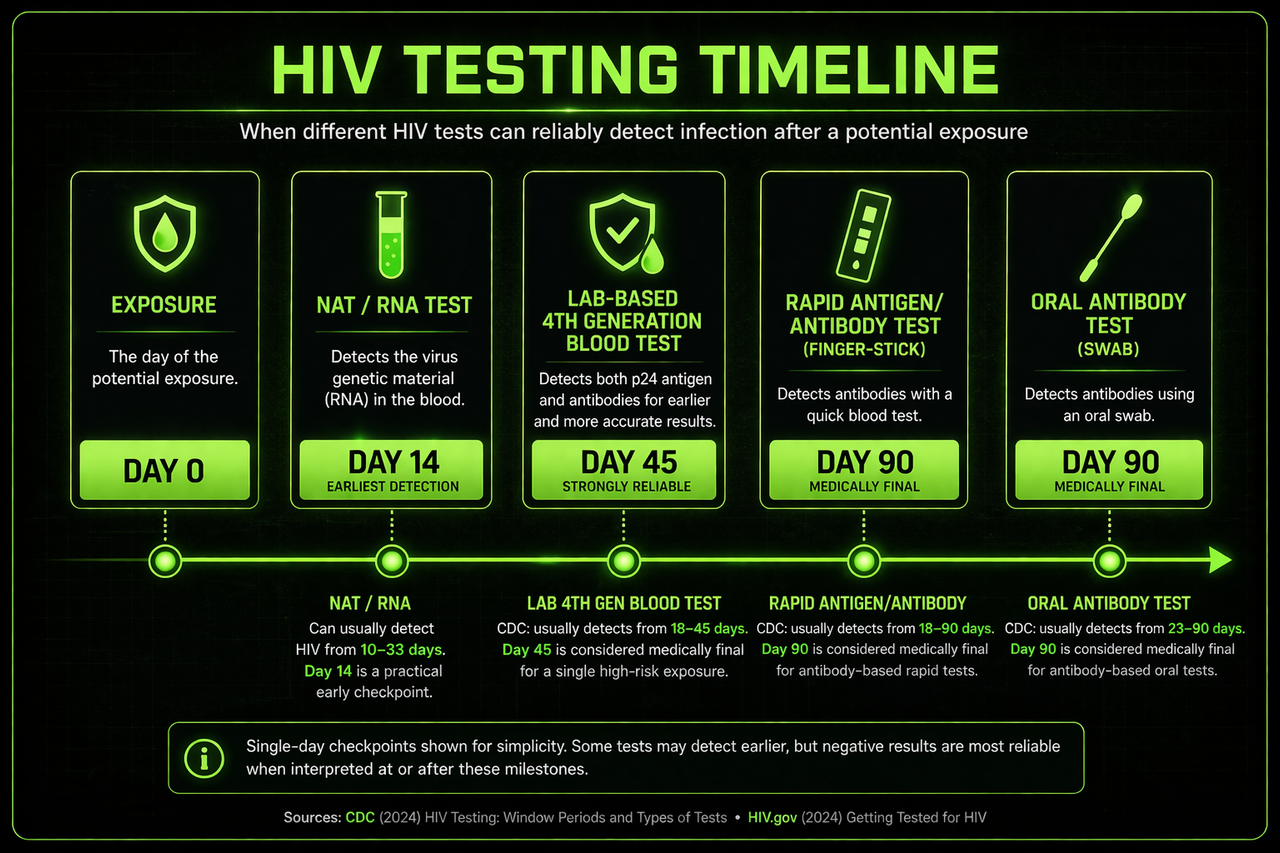
OraQuick and similar oral swab tests
- Begin to detect many infections around three weeks after exposure.
- Considered conclusive at twelve weeks for most guidelines.
Fourth generation blood tests
- Detect many infections around fourteen days after exposure.
- Usually considered conclusive at forty five days for a single high risk event.
PCR or RNA tests
These tests detect viral genetic material directly and can identify infection earlier than antibody or antigen tests. They are not routinely recommended for standard screening, but they may be used in specific high risk or clinical situations.
Your HIVRISKREPORT output calculates personalized earliest and conclusive testing dates based on the exact date of your encounter and the type of test you plan to use.
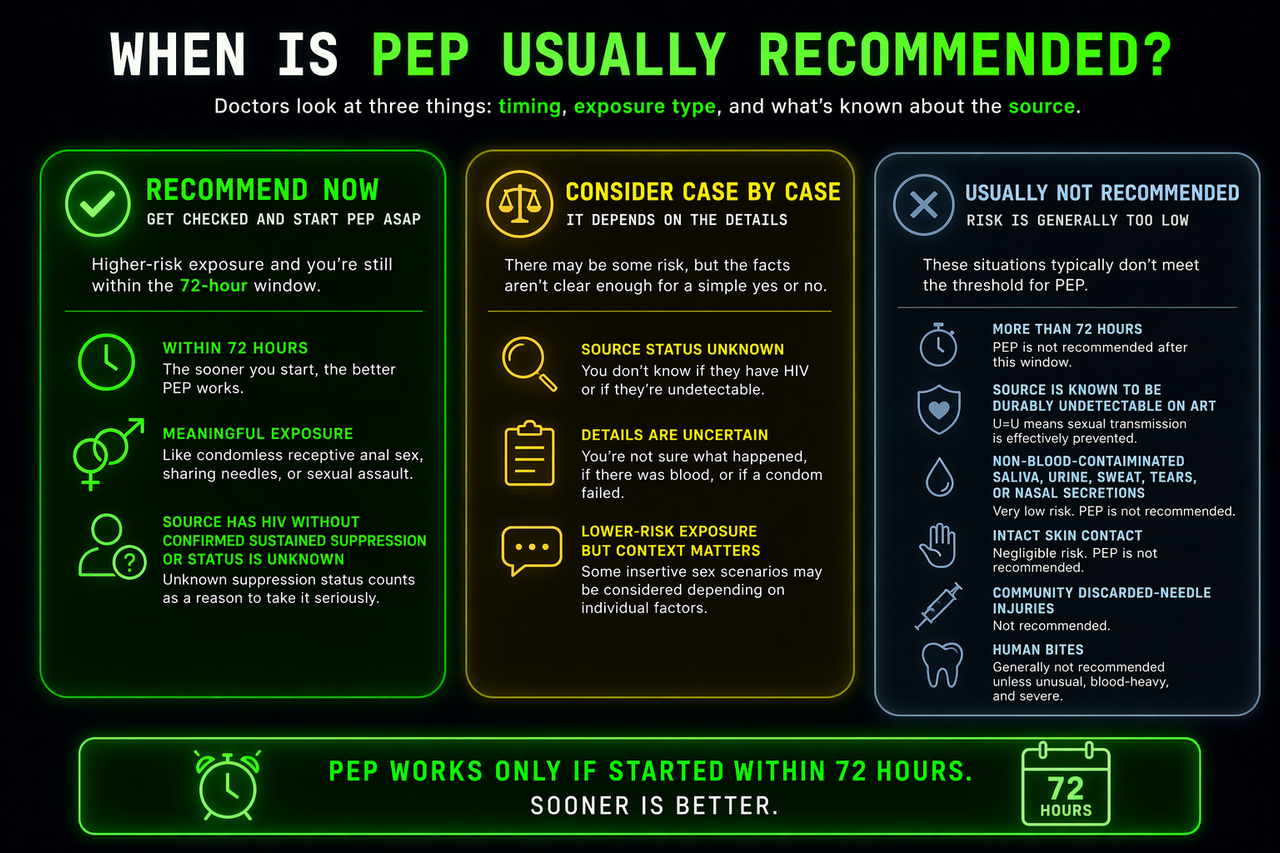
PEP: Emergency HIV Prevention After Exposure
Post Exposure Prophylaxis, often shortened to PEP, is a course of HIV medication that can reduce the chance of infection after a high risk exposure. It is time sensitive and must be started quickly.
- PEP must be started within seventy two hours of the exposure.
- It is most effective when started within the first twenty four hours.
- It is usually recommended for specific higher risk situations such as unprotected receptive anal sex with a partner known to be HIV positive or in a high risk group.
If your encounter was more than seventy two hours ago, PEP is no longer an option. In that case the focus shifts to accurate testing at the right times, which your personalized report can help you plan.
Always speak to a local sexual health clinic or emergency department if you think you may need PEP. This site does not replace medical advice.
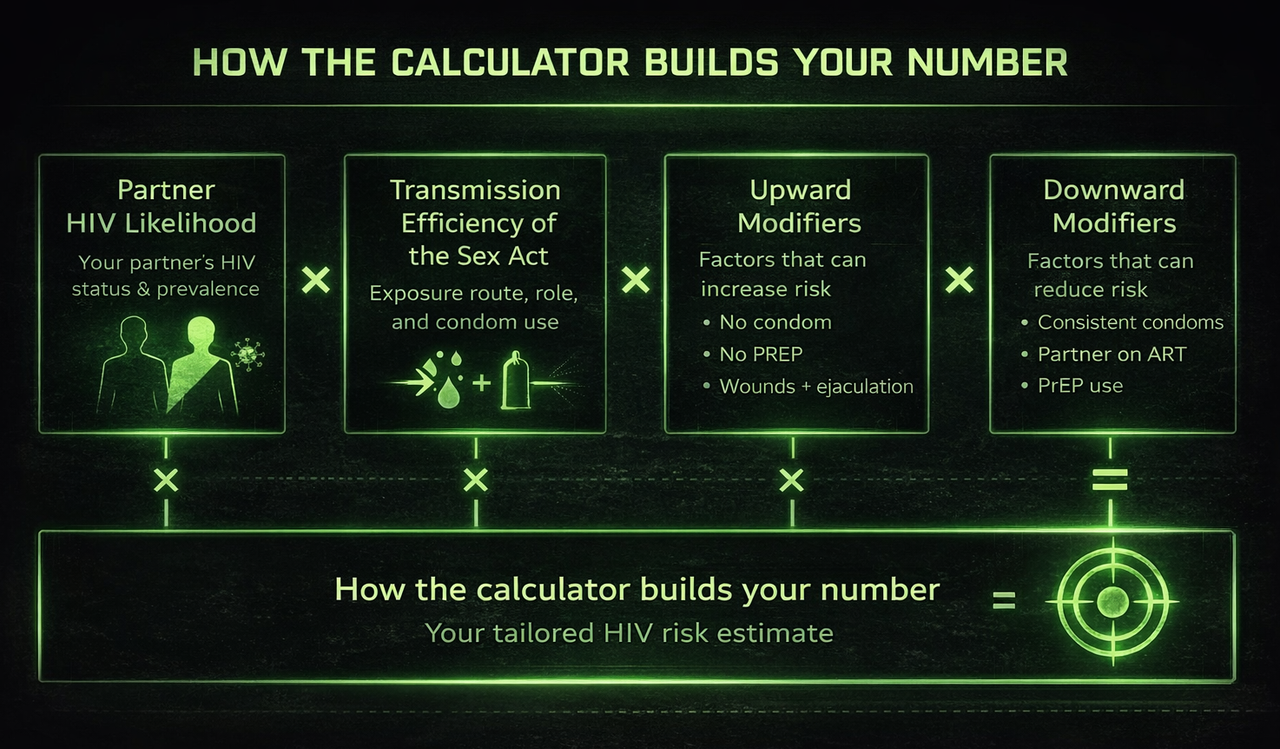
What Determines HIV Risk?
HIV risk can be estimated by analysing a number of different variables. Although testing is the only way to know your true status, knowing the risk transmission probability of a single encounter can help bring realistic context and reduce uncertainty. It comes down to two questions: could your partner have HIV, and if so, how efficient was the exposure? Everything else is a modifier that pushes the estimate up or down. If you want the number for your exact encounter, you will need a personalized calculation.
What determines risk:
How common HIV is in your partner’s context, plus how likely treatment has reduced infectiousness.
The type of sex and your role, because different tissues transmit differently.
Condoms, PrEP, ejaculation location, and signs of irritation or other infections.
1) Partner HIV status and prevalence
The starting point is simply: what is the chance your partner has HIV in the first place? That varies by setting and network, so we estimate it from epidemiological data that matches what you report.
- Location: country and sometimes region-level differences.
- Demographics: gender and the relevant sexual network.
- Context: risk factors you report or do not report.
- Treatment reality: when status is unknown, we account for how often people are diagnosed, on ART, and virally suppressed.
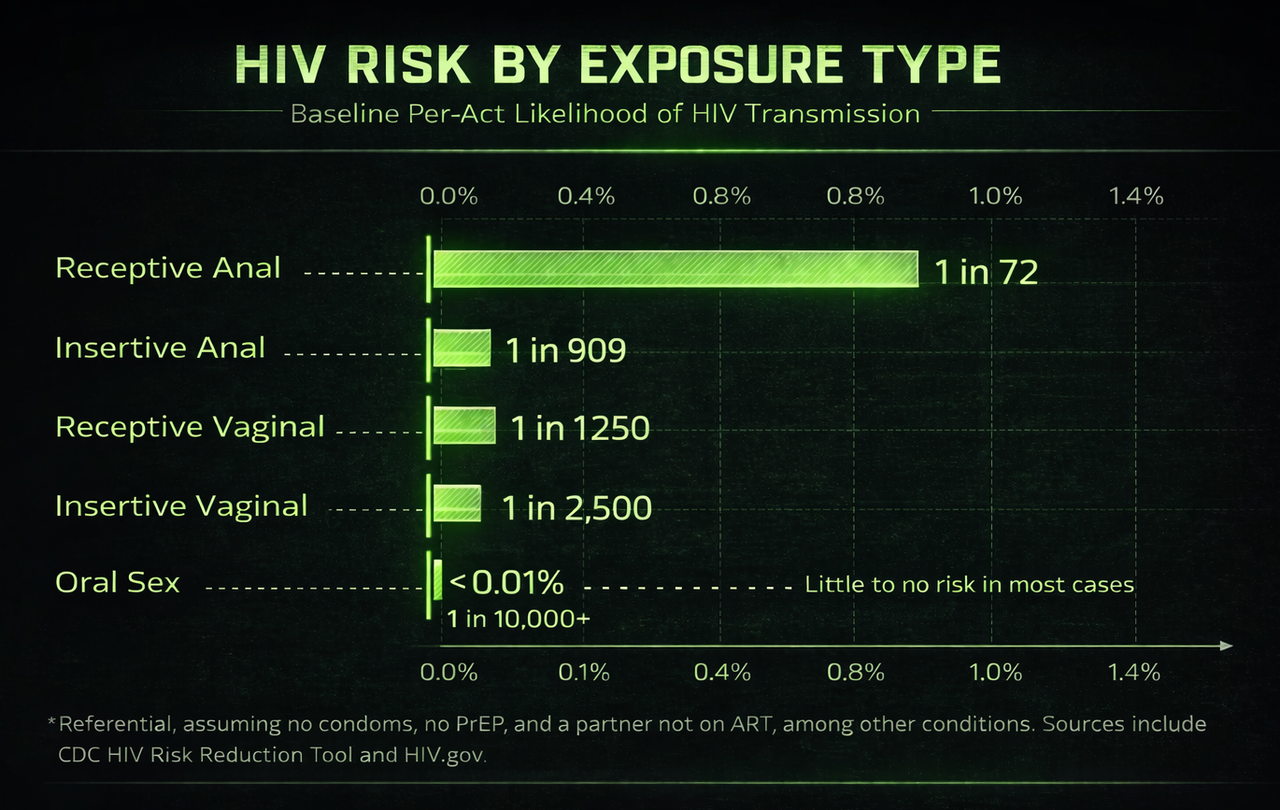
2) Type of sex and role
Not all exposure routes have the same efficiency. In general, mucosal tissue that is thinner and more prone to micro-tears carries higher per-act risk, especially without barriers.
- Receptive anal: typically the highest per-act risk.
- Insertive anal: lower than receptive anal, but not “nothing”.
- Vaginal sex: generally lower than anal, with differences by role.
- Oral: usually low to negligible in most circumstances.
- Non-penetrative contact: effectively zero for HIV in normal scenarios.
3) Condoms and what happened to them
Condoms are one of the most reliable downward modifiers when used correctly and they stay intact. The detail that matters is not intention, it is what actually happened.
- If it stayed on and did not break or slip, the estimate drops substantially.
- If it broke, slipped off, or was not used, the calculation reflects unprotected exposure.
- If you are unsure, your report shows how uncertainty affects the result.
4) Viral load, ART, and the U equals U effect
Viral load is the biggest swing factor once someone actually has HIV. When a person is on ART and maintains an undetectable viral load, sexual transmission does not occur. That is the science behind U equals U.
- Known HIV-positive partner on effective ART: the estimate collapses towards zero.
- Unknown status: we use country-level treatment and suppression patterns to avoid unrealistic assumptions.
5) Wounds, inflammation, and other infections
Cuts, sores, significant irritation, or an active STI can increase susceptibility because the barrier is compromised. This matters most when there is unprotected anal or vaginal exposure.
- We ask simple questions so you can include this without over-explaining.
- If you prefer not to share, the report stays conservative and transparent about assumptions.
6) Why a personalized report is different
Most articles stop at generalities. Your report shows the actual numbers, the assumptions, and how each input moves the estimate. You should be able to look at the result and understand why it is that number.
- A clear probability in percent and “1 in X”.
- A step-by-step explanation, not a generic reassurance.
- Practical next steps that fit the risk tier.
Why general articles can’t answer your question
Most HIV websites are written to be broadly true, but not personally accurate. They have to cover every country, every partner profile, and every type of exposure, so the data stays deliberately general. Your question is more specific: what does this mean for my exact encounter? The answer depends on concrete inputs such as local prevalence, your role, what actually happened with protection, real-world treatment and viral suppression, and whether there were cuts or irritation. When any of these details are guessed or misunderstood, people often end up in the worst of both worlds: unnecessary panic, or false reassurance. A personalized calculation replaces guesswork with a transparent, step-by-step estimate, giving you a clear probability, the assumptions behind it, and next steps matched to your risk tier.
What Goes Into Your Personalized Calculation
Generic HIV risk calculators cannot tell you what your specific encounter means, because they ignore the exact inputs that change the maths. A personalized report takes your answers, maps them to evidence-based baseline rates, then applies only the modifiers that your scenario actually earns.
| Variable we use | Why it matters in the calculation |
|---|---|
| Date of encounter | Anchors all timing guidance, including when testing becomes reliable and whether PEP could still be time-relevant. It also keeps the assessment tied to one specific event, rather than a vague timeframe. |
| Country of encounter | Determines the baseline prevalence estimates and treatment cascade assumptions we use in the model. HIV rates, diagnosis coverage, and viral suppression vary meaningfully by country, which can move the final estimate up or down. |
| Your gender | Helps select the correct baseline prevalence context and ensures the per-act transmission estimates match the anatomy and exposure route relevant to you. |
| Partner’s gender | Used alongside location to choose the correct partner prevalence estimate and to match the correct per-act transmission pathway. |
| Partner known HIV-positive | If the partner is confirmed positive, the model shifts focus to treatment and viral load. If status is unknown, the report estimates the likelihood they have HIV based on epidemiological data. |
| Type of sexual activity | Sets the baseline per-act transmission probability. Vaginal, anal, and oral exposures have very different statistical risk profiles. |
| Your role: insertive or receptive | Selects the correct per-act risk within the sex type. Receptive and insertive roles are not interchangeable in the maths. |
| Condom use | Applies a major downward modifier when a condom was used properly and stayed intact. If no condom was used, the model treats the exposure as unprotected. |
| Partner injection drug use or other major risk factors | Adjusts the estimated likelihood that the partner has HIV when additional high-exposure risk factors are present. |
| Sex worker encounter | Changes the prior probability of exposure because certain occupational contexts have statistically different prevalence patterns. The model treats this as a partner-likelihood modifier, not a moral judgement. |
| Partner had multiple partners recently | Used as a context signal that can increase exposure probability in some scenarios. When unknown, the report stays conservative and explains how uncertainty affects the estimate. |
| Ejaculation inside the body | Influences exposure intensity because semen can carry HIV when viral load is not suppressed. This is treated as an upward modifier in unprotected vaginal or anal sex. |
| Partner on HIV treatment: ART | Treatment status is one of the biggest swing factors if the partner has HIV. Effective ART that results in viral suppression can reduce transmission risk to effectively zero. |
| You take PrEP | Applies a strong downward modifier because PrEP meaningfully reduces acquisition risk when taken correctly. |
| Wounds or inflammation | Cuts, sores, irritation, or active STIs can increase susceptibility by compromising tissue barriers, especially in unprotected anal or vaginal sex. |
| Circumcision status | Considered only when it is biologically relevant to the exposure route. If it does not apply, the model keeps it neutral and explains why. |
| Personalized content analysis | A plain-language layer that converts the maths into an understandable explanation, flags the variables that drove your result, and points you towards the next best action for your risk tier. |
This is why two people can have the “same” type of sex but end up with different real-world risk. The personalized report does not rely on generic labels. It shows the inputs, the assumptions, and the step-by-step logic behind the final number.
Why You Can Trust This Tool
HIVRISKREPORT was created because anxiety after a sexual encounter can become overwhelming. People search the internet, see worst-case stories, and struggle to think clearly. Putting numbers on the situation does not erase risk, but it can help bring fear down to something more manageable.
The model behind the report is based on published research rather than guesswork. Key sources include:
- Per-act HIV transmission risk meta-analyses.
- Country-level prevalence and treatment coverage data from organisations such as CDC and UNAIDS.
- Studies on condom effectiveness, PrEP, ART, and viral suppression.
You remain anonymous when you use the tool. The goal is to provide clarity and structure to a situation that often feels chaotic and frightening.
“A great counterweight to all the panic posts on Reddit. It greatly reduced my anxiety related to a recent “incident” and I am forever grateful that you took the time and effort in creating this service.”
When your brain will not switch off
If you keep replaying the encounter in your head and swinging between “I am fine” and “what if I ruined my life”, this guide and the calculator give you one clear framework instead of endless mental loops.
When Google made it worse
You might have opened ten tabs, seen horror stories and vague odds, and walked away more confused. Here you get a single, calm explanation built from real data, all in one place.
When you need a plan, not more panic
Instead of guessing or waiting in fear, you leave with a clear understanding of what drives risk, when to test, and how a personalized report can turn “what if” into “here is what I will do now”.
Get Your Personalized HIV Risk Report
This guide explains the general rules of HIV transmission. Your personalized report takes the next step and applies those rules to your exact encounter, turning vague fear into a single, clear number you can understand and act on.
What your report includes
Personalized Risk Analysis
- A fully personalized, 6-page HIV risk assessment based on your partner, country, type of sex, role, condom use, ART or PrEP, wounds, ejaculation, duration, and more.
- Partner HIV probability modelling using country and group-specific data rather than generic averages.
- All upward and downward modifiers clearly listed, including condoms, ART, PrEP, circumcision, wounds, and type of sex.
Clear, Step-by-Step Explanation
- A plain-language walkthrough showing exactly how each part of your encounter affects risk.
- Your final risk shown four ways: percentage, decimal, fraction, and a simple “1 in X” format.
- A “what helped and what hurt” summary highlighting which factors lowered risk and which increased it.
Testing & Next Steps
- A personalized testing timeline with earliest and conclusive dates for RNA tests, 4th generation blood tests, and at-home oral tests.
- A clear next-step plan so you know exactly what to do after reading your report.
- Risk-tier specific FAQ answers tailored to your actual probability, not generic advice.
Perspective & Reassurance
- Real-world comparisons that place your risk alongside everyday events and other common STIs.
- A brief alternative scenario showing how risk would change if one key detail were different.
- Emotional reassurance written for people experiencing panic or health anxiety.
Your report is generated as a confidential, password-protected PDF that you can save to your device and read in private. No account, no sign-up, and no sharing of your name.
More HIV Risk and Testing Resources
Disclaimer
HIVRISKREPORT is an informational and educational tool. It does not replace medical advice, diagnosis, or treatment from a qualified healthcare professional. If you think you may have been exposed to HIV, or if you feel unwell, contact a sexual health clinic, your doctor, or an emergency service in your area.