HIV Symptoms: Separating Fact From Fear
A calm, evidence-based guide to understanding what early HIV symptoms really look like.
🕓 Last updated: 10th April 2026
Symptoms cannot tell you whether you have HIV.
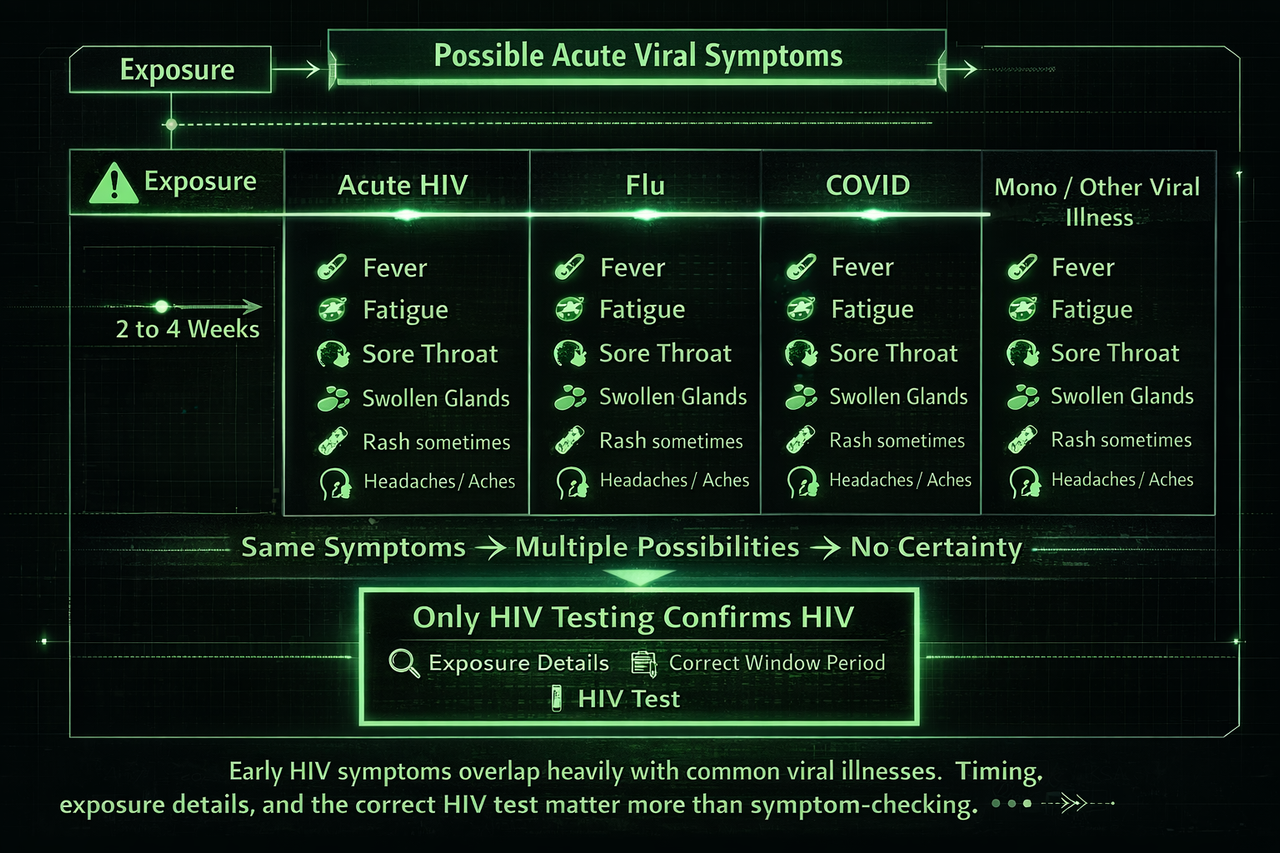
Early HIV symptoms, when they happen, often look like a short flu-like illness 2 to 4 weeks after a higher-risk event. That exact pattern is also seen with flu, mono, COVID, strep, and many common infections.
The only way to know your status is an HIV test taken at the correct window period.
If you want a personalised risk estimate based on your exact encounter, you can get one below. It is based on exposure details and published evidence, not symptoms.
If you are reading this, you are probably stressed and scanning your body for signals, a warm feeling, a headache, a throat tickle, and wondering if it means HIV. Many people deal with this same fear everyday, but it's important to know that symptoms are a very poor way to measure risk. If you want a grounded next step, use the risk assessment to turn panic into a plan.
The acute stage: what early HIV symptoms actually look like
When they happen, early HIV symptoms (ARS) often show up about 2 to 4 weeks after infection and usually last under a week. If you are trying to time your testing, use our HIV test window periods guide.
Fever
In acute HIV, fever is usually moderate and lasts a few days. It feels like a typical viral fever, similar to flu or COVID, and is not a unique pattern.
Fatigue
People describe a heavy, whole-body tiredness that does not improve with one night’s sleep. This also appears with many viral infections.
Sore throat
Usually general soreness, not sharp one-sided pain. It can look exactly like a viral sore throat or mild strep.
Swollen lymph nodes
Often on both sides, slightly enlarged, rubbery, and tender. This also happens with colds, strep, flu, mono, and many other infections. If this is your main fear, read our deeper guide on HIV and swollen lymph nodes.
Rash
A flat or slightly raised red rash, usually not itchy. Often on the chest, back, or upper arms, and it can resemble rashes from common viral illnesses.
Muscle and joint aches
General aching similar to flu or COVID. Nothing about the pattern is uniquely HIV.
Headaches
Usually dull or pressure-like. Similar to dehydration, stress, or common viral headaches.
Night sweats
Waking up damp or needing to change clothes. This can also be caused by stress, flu, sleep cycles, and anxiety.
Key reminder: None of these symptoms are HIV-specific. They occur in far more people without HIV than with it.
Testing is the only signal you can trust. If you want the simplest timing framework, start with our window periods.
Why symptoms are a poor HIV calculator
Many people have zero symptoms
A large portion of people who acquire HIV feel totally normal in the first month. No symptoms does not mean negative. This is why the testing timeline matters more than feelings. See when results are reliable.
Symptoms overlap with dozens of common infections
Clinicians do not diagnose HIV from symptoms alone. They rely on exposure details and testing because the overlap is huge.
Anxiety can create or amplify symptoms
Stress can cause headaches, warmth, throat tightness, fatigue, and sleep disruption. That can happen even without an infection. If your worry is driven by myths about casual contact, read can HIV live outside the body?
Get a personalised transmission probability and a testing timeline with exact dates, based on your exact encounter. If you want to understand the logic behind the calculator, start here: how the risk calculator works.
Frequently asked questions
Can symptoms alone tell me if I have HIV?
No. Symptoms overlap with flu, mono, strep, colds, COVID, stomach bugs, and anxiety. Even clinicians cannot diagnose HIV from symptoms alone. HIV status is confirmed by testing at the right time.
How soon after exposure would HIV symptoms appear?
When symptoms happen, they are most commonly reported around 2 to 4 weeks after infection. Symptoms the next day, or within a few days, are far more likely to be stress, a different infection, or normal body noise. If you are planning your test, use the window period timeline.
What does an acute HIV rash look like?
Rash can happen in acute infection, but it is not specific. Many viral illnesses can cause rashes. When described, it is often:
- Flat or slightly raised red spots.
- Often on the torso, upper arms, or back.
- Sometimes not itchy, but itchiness can still occur for other reasons.
The key point is this: rash does not confirm HIV. Testing does.
If I have swollen lymph nodes, does that mean HIV?
Not by itself. Lymph nodes swell from common infections and inflammation, and they can also feel more noticeable when you are repeatedly checking them. If this is the symptom you are fixating on, see our lymph node guide. Exposure details and test timing matter far more than a single symptom.
Can anxiety cause symptoms that feel like HIV?
Yes. Anxiety can drive real physical sensations. Common ones include:
- Heat sensations, flushing, sweating, or chills.
- Throat tightness, chest tightness, and shortness of breath.
- Headaches, fatigue, stomach upset, and poor sleep.
If you are spiralling, the highest value move is a testing plan, not symptom checking. Start with window periods, then map it to your dates.
What if I had symptoms, but my exposure was low-risk?
In that situation, symptoms become even less informative. Low-risk exposures are far more likely to be followed by unrelated illness or anxiety-driven symptoms. If you want certainty, follow the correct testing window for your test type. If your exposure was oral, see HIV risk from oral sex.
If I used a condom, should I still worry about symptoms?
Condoms dramatically reduce HIV transmission risk when they are used correctly and do not break. Symptoms after a protected encounter are much more likely to be unrelated, but testing can still provide peace of mind if you are anxious. If you want a tailored probability and timeline anyway, use the assessment.
If my partner is on treatment and undetectable, do symptoms matter?
Effective treatment that keeps viral load undetectable greatly reduces the risk of transmission. Symptoms still cannot confirm anything. If you want the simplest explanation of this, see viral load and U=U. If you are unsure about your situation, the most grounded path is a test at the correct time.
What test should I take and when?
Test timing depends on the test type. A simple framework:
- 4th generation blood test: reliable around 28 days, often treated as conclusive by 45 days in many guidelines.
- RNA (PCR) test: can detect earlier in some cases, but usually needs a follow-up 4th generation test.
- Oral swab antibody tests: longer window, often treated as conclusive at 90 days.
If you want this mapped to your exact dates, start with our window period guide, or generate your personalised timeline in the assessment.
Should I consider PEP after an exposure?
PEP is time-sensitive and is typically discussed when the exposure is higher-risk and within 72 hours. If you are inside that window and worried, it is worth speaking to a clinician or urgent care service quickly. If you want the difference explained clearly, see PEP vs PrEP.
I tested negative but still have symptoms. What now?
A negative test is reassuring when it is taken at the correct time for that test type. If symptoms continue:
- Consider that another infection is more likely than HIV.
- Use the appropriate follow-up test window if you tested early.
- See a clinician if symptoms are severe or persistent.
If you are not sure whether your test was early or conclusive, check your test type against window periods.
What symptoms should make me seek urgent medical care?
This page is educational, not medical advice, but urgent care can be appropriate if you have:
- Severe chest pain, trouble breathing, fainting, or confusion.
- High fever that persists, severe dehydration, or worsening severe pain.
- Any symptom that feels dangerous or rapidly getting worse.
What should I do next if I am spiralling?
Make it actionable. Stop symptom scanning and run a simple plan:
- Identify the exposure details and approximate date.
- Choose the right test type and the correct timing window.
- Get a personalised risk estimate so you are not guessing.
A good first move is the calculator guide, then the assessment.