HIV Rash: What It Looks Like vs Common Skin Conditions
An evidence-based clinical guide to acute HIV rash presentation, differential diagnosis from common dermatological conditions, and the role of exposure assessment and testing.
A rash alone cannot confirm or exclude HIV.
An acute HIV rash is typically widespread, symmetrical, and maculopapular, characterised by flat discolourations interspersed with small raised papules. It most commonly presents on the trunk and coincides with systemic symptoms such as fever, pharyngitis, fatigue, or lymphadenopathy.
Urticaria, miliaria, contact dermatitis, eczema, and friction-related irritation are far more prevalent causes of skin changes after sexual contact.
What an acute HIV seroconversion rash typically presents as
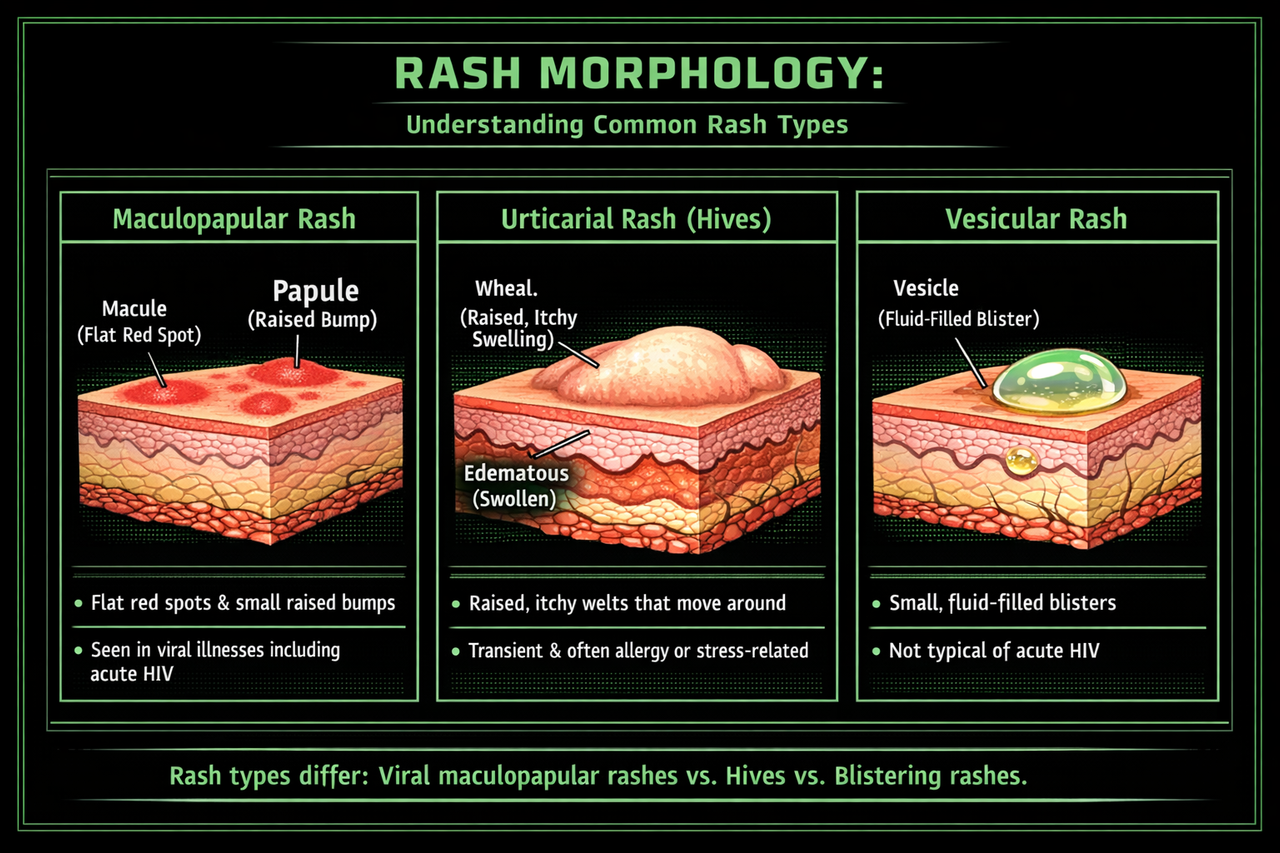
The exanthem associated with acute HIV infection is most commonly described in clinical literature as morbilliform or maculopapular: a combination of macules (flat colour changes) and papules (small raised lesions). It is characteristically widespread and symmetrical, most often involving the trunk.
Typical clinical features
- Distribution: Most often originates on the chest, back, or abdomen with potential extension to the extremities.
- Symmetry: Characteristically bilateral and relatively uniform.
- Morphology: Flat macules interspersed with small papules, not vesicular or bullous.
- Duration: Typically persists for several days. Clinical reports commonly describe 5 to 8 days.
Associated systemic features
The acute retroviral syndrome presents with non-specific features that overlap considerably with other viral illnesses. Commonly reported accompaniments include fever, fatigue, myalgia, pharyngitis, lymphadenopathy, and the exanthem.
When a rash following sexual contact is the sole finding, particularly in the absence of a meaningful exposure risk, common dermatological conditions represent a far more probable explanation. Clinical decision-making should be guided by exposure history and appropriate testing rather than visual pattern-matching alone.
A common misconception encountered online is that "HIV rash is never itchy." Clinical reality is more nuanced. Acute HIV exanthems can produce pruritus or irritation, and the presence or absence of itch alone is insufficient to confirm or exclude any diagnosis. The more diagnostically relevant features are lesion morphology, distribution pattern, temporal behaviour, presence of systemic symptoms, and most critically, the nature of the preceding exposure.
Differential diagnosis: common conditions that mimic HIV rash
The majority of skin changes that prompt concern are attributable to common, benign dermatological conditions. Perspiration, psychological stress, new topical products, mechanical friction, and hormonal fluctuation all produce skin changes that can appear alarming in the context of health anxiety. The following are the most frequently encountered differentials.
Urticaria (hives)
Urticaria presents as raised wheals that are typically pruritic and can appear dramatic. The distinguishing behavioural characteristic is transience: individual lesions typically resolve within 24 hours at any given site before potentially reappearing elsewhere.
- Migratory pattern: Lesions resolve in one location and emerge at another.
- Pruritus: Often intense and a dominant feature.
- Triggers: Stress, intercurrent infections, dietary factors, medications, thermal changes, pressure, and frequently idiopathic.
Miliaria (heat rash)
Miliaria results from eccrine duct obstruction or inflammation. It characteristically presents in hot, humid conditions, following perspiration, or in areas of occlusion from tight clothing.
- Distribution: Clustered papules in areas prone to sweating, including the neck, chest, back, and skin folds.
- Sensation: Prickling or pruritus is common, particularly in miliaria rubra.
- Resolution: Typically improves with cooling and reduced occlusion.
Contact dermatitis and eczema
Irritant or allergic contact dermatitis can develop following exposure to new topical agents, including soaps, barrier contraceptives, lubricants, laundry detergents, fragrances, or depilatory products. Eczematous patterns tend to be pruritic, patchy, and may be scaly or xerotic.
- Distribution correlates with exposure: Localised to areas of contact with the offending agent.
- Pruritus and inflammation: Typically prominent features.
- Chronicity: Often recurrent in previously affected areas.
Other viral exanthems and drug eruptions
Numerous viral infections produce generalised maculopapular rashes. Medication reactions represent another common cause. In the immunocompromised population, dermatological manifestations can have multiple aetiologies including the underlying condition, co-infections, and therapeutic agents.
If a rash develops following initiation of any new medication, particularly if accompanied by facial oedema, mucosal involvement, or blistering, this warrants prompt medical evaluation regardless of HIV concerns.
Temporal relationship: why timing supersedes visual assessment
The acute retroviral syndrome, when clinically apparent, typically manifests within approximately 2 to 6 weeks following acquisition. This temporal framework is precisely why a rash appearing within hours or 1 to 2 days of a low-risk encounter is far more consistent with common dermatological conditions than with acute HIV infection.
If you would like to understand whether your timeline is consistent with acute HIV, a structured exposure and timing assessment can provide that context.
The axillary rash scenario
Axillary rashes are among the most common triggers for health anxiety because the area feels anatomically significant, is warm, densely populated with eccrine glands, and subject to considerable friction. However, an isolated axillary rash is far more frequently attributable to local dermatological factors than to acute systemic HIV infection.
Benign conditions that preferentially affect the axillae
- Intertrigo: Friction and moisture-related inflammation of the skin fold.
- Contact dermatitis: Reaction to deodorants, antiperspirants, fragrances, or preservatives.
- Folliculitis or pseudofolliculitis: Secondary to shaving or depilation.
- Candidiasis: Yeast overgrowth in the warm, occluded environment.
- Miliaria: Eccrine duct obstruction from perspiration in covered areas.
These conditions are common precisely because the axillary microenvironment favours irritation and microbial overgrowth. This is normal dermatological physiology, not a marker of systemic infection.
Why isolated axillary involvement is atypical
The acute HIV exanthem, when present, is characteristically widespread and symmetrical, with predominant truncal involvement. It typically co-presents with systemic features including fever, fatigue, pharyngitis, and lymphadenopathy.
A rash confined to one axilla, localised to skin folds, or clearly temporally related to a change in deodorant, increased perspiration, or shaving is far more consistent with a local dermatological explanation than with acute retroviral syndrome.
The evidence-based approach to this scenario is straightforward: the rash itself is not the determining factor, the exposure history is. If there was no meaningful transmission risk (for example, no penetrative sexual contact, or consistent barrier protection was used), an isolated axillary rash does not constitute a clinical basis for suspecting HIV.
If a genuine higher-risk exposure did occur and the individual is within the 2 to 6 week window, visual assessment of the skin is not the appropriate diagnostic pathway. A structured testing plan based on correct timing and test selection is the evidence-based approach.
Most axillary rashes are self-limiting, but the following warrant clinical assessment:
- Significant pain, spreading erythema, warmth, or oedema: possible bacterial cellulitis or abscess.
- Purulent discharge, recurrent boils, or painful nodules: folliculitis, abscess, or hidradenitis suppurativa.
- Systemic features: fever or malaise accompanying a rapidly progressive rash.
- Blistering, desquamation, mucosal ulceration, or facial oedema: urgent assessment indicated.
These are general dermatological and medical red flags, not indicators specific to HIV. They warrant prompt evaluation on their own merit.
- 0 to 72 hours post-exposure: More consistent with immediate hypersensitivity, urticaria, friction, miliaria, irritant reaction, or coincidental viral illness.
- 1 to 2 weeks: Generally earlier than the typical window for classic acute retroviral syndrome presentation, though individual variation exists.
- 2 to 6 weeks: The interval during which clinicians maintain higher suspicion for acute HIV, provided there was a genuine exposure risk and a compatible clinical syndrome.
If you are trying to contextualise a specific skin change following a specific encounter, a private exposure assessment can help you understand where the evidence points.
Pathophysiology: why acute HIV can produce an exanthem
Acute HIV infection represents a period of rapid viral replication and intense immune activation prior to the establishment of adaptive immune control. This immunological response can manifest as a viral exanthem, a mechanism shared with numerous other systemic viral infections.
Histopathological examination of acute HIV exanthema demonstrates relatively non-specific findings: a superficial perivascular lymphocytic infiltrate without pathognomonic features. This supports the understanding that the rash reflects downstream immune activation rather than a unique, HIV-specific dermatological signature.
The clinical implication is clear: because the rash lacks specificity, it cannot serve as a reliable standalone diagnostic indicator. This is precisely why evidence-based clinical guidance prioritises laboratory testing over symptom monitoring.
Recommended approach if you have concerns
Assess exposure risk objectively
The rash does not define risk; exposure history does. If the encounter was low-risk (no penetrative contact, or consistent barrier method use), common dermatological conditions are overwhelmingly more probable. If the encounter carried genuine transmission risk, the appropriate response is structured testing and clinical guidance rather than self-diagnosis from skin appearance.
Use the appropriate test at the appropriate interval
Acute HIV infection cannot be diagnosed clinically. It requires laboratory confirmation. The acute phase is defined by the interval during which HIV RNA is detectable but antibody responses may be incomplete, which is why both test selection and timing are critical variables.
If you are within a genuine window of concern following a higher-risk exposure, consultation with a sexual health clinician regarding an appropriate testing strategy is the evidence-based next step.
Stress and anxiety are well-established exacerbating factors for urticaria, miliaria, and various inflammatory dermatoses. Repetitive self-examination of the skin perpetuates anxiety because normal physiological variation in skin appearance is misinterpreted as pathology. The disciplined approach is to focus on objective data: what was the actual exposure risk, and what does the appropriate testing timeline indicate? These are the inputs that provide genuine clinical clarity.
Red flags: when any rash requires urgent medical assessment
- Respiratory difficulty, lip or tongue oedema, or widespread facial swelling (anaphylaxis).
- Blistering, skin desquamation, or painful rash, particularly with concurrent fever (possible Stevens-Johnson syndrome or toxic epidermal necrolysis).
- Oral, ocular, or genital ulceration accompanied by systemic illness.
- Rapidly spreading non-blanching purpura, severe headache, nuchal rigidity, or acute deterioration in clinical condition.
These represent general medical emergencies. They are not specific indicators of HIV and require prompt assessment irrespective of any sexual health concerns.
Want clarity based on your specific situation?
Our private assessment evaluates your exposure details, timing, and symptoms against clinical evidence, providing a structured, personalised understanding of where you stand and what testing (if any) would be appropriate.
Private. Evidence-based. No account required.
Frequently Asked Questions
It is characteristically described as a symmetrical, generalised maculopapular or morbilliform exanthem with predominant truncal involvement. It typically co-presents with systemic viral features and persists for days rather than appearing and resolving within hours.
It can be pruritic, but pruritus is not a reliable diagnostic discriminator. Urticaria is more characteristically intensely pruritic and transient, whereas the acute HIV exanthem tends to be a sustained maculopapular pattern. Clinical testing remains the definitive approach regardless of symptom character.
The typical temporal window for acute retroviral syndrome is measured in weeks, not hours. Rashes appearing within 24 to 48 hours are far more consistent with contact allergy, urticaria, miliaria, mechanical irritation, or coincidental dermatological conditions. If a genuine higher-risk exposure occurred, an appropriate testing strategy based on correct timing is more informative than symptom interpretation.
The hallmark of urticaria is the transient nature of individual lesions: wheals that resolve within 24 hours at any given site before potentially emerging elsewhere. This migratory, short-lived pattern is highly characteristic.
No. The clinical features of acute HIV overlap substantially with numerous common conditions. Definitive diagnosis requires laboratory testing. If there is genuine concern based on exposure history, a structured testing plan is the evidence-based path to certainty.
Sources & References
- HIV.uw.edu, Acute and Recent HIV Infection, rash pattern (maculopapular, trunk) and testing principles: hiv.uw.edu
- NIH HIVinfo, HIV and Rash fact sheet: hivinfo.nih.gov
- DermNet NZ, Acute HIV infection syndrome (rash distribution): dermnetnz.org
- DermNet NZ, Urticaria overview, wheals typically resolve within 24 hours: dermnetnz.org
- DermNet NZ, Miliaria, eccrine duct obstruction: dermnetnz.org
- NCBI Bookshelf (StatPearls), Miliaria overview: ncbi.nlm.nih.gov
- Matsumoto et al. (2022), Acute HIV case review, rash frequency and typical duration: PMC9828947
- Balslev et al. (1990), Histopathology of acute HIV exanthema: PubMed 2332516
This article is intended for educational purposes and does not constitute personal medical advice or diagnosis. If you believe you have had a higher-risk exposure, or if you are experiencing a severe rash or systemic symptoms that concern you, please contact a clinician or sexual health service for individualised guidance.