Receptive vs insertive: what the words mean
You are the partner receiving penetration. For anal sex, that means rectal tissue is exposed to partner fluids.
You are the partner penetrating. For anal sex, penile tissue is exposed. The opposite of receptive is insertive.
These words describe exposure surfaces and biology, not identity or morality.
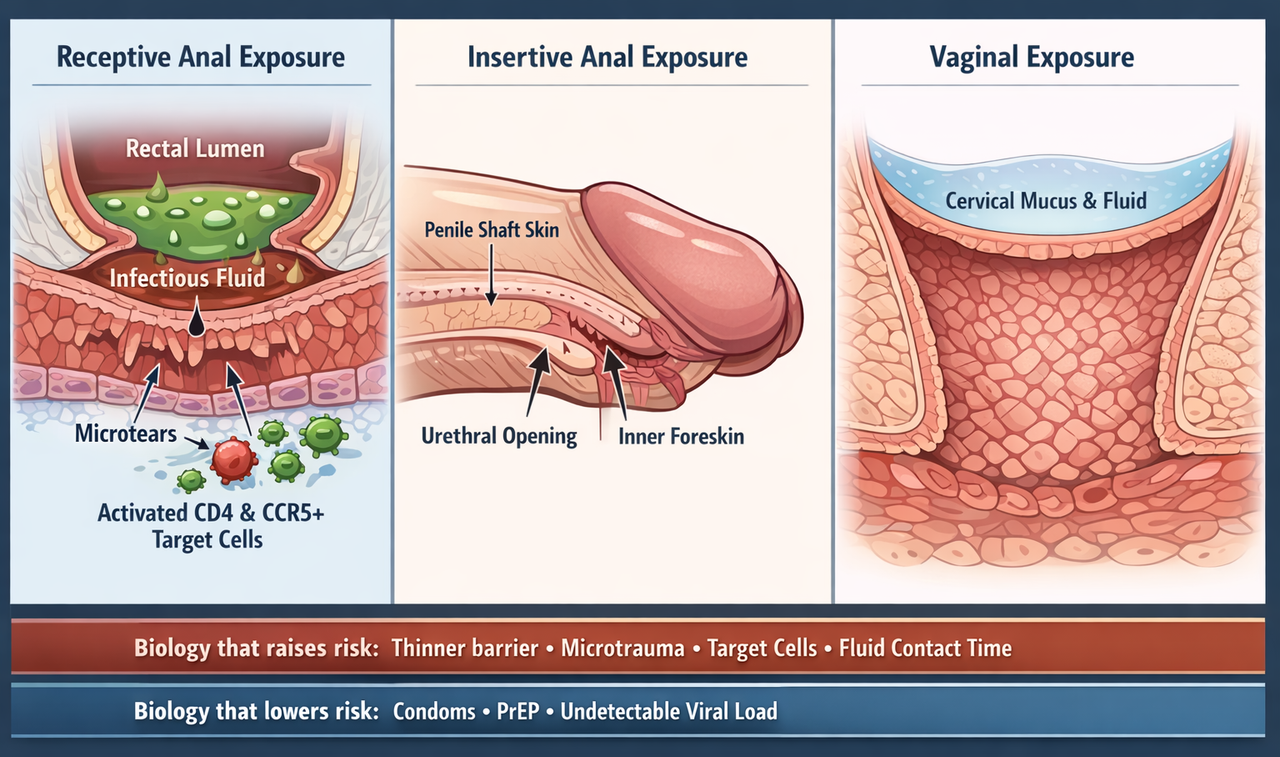
Tissue structure helps explain why receptive anal exposure carries the highest baseline per-act HIV risk. Thinner barrier tissue, microtrauma, target-cell access, and fluid contact all affect susceptibility.
Baseline per-act numbers (what they mean, and what they assume)
The most widely cited per-act estimates used by major public health sources are below. These numbers are best thought of as population averages under a specific set of assumptions.
| Exposure type | Per 10,000 exposures | Percentage | 1 in X |
|---|---|---|---|
| Receptive anal sex | 138 per 10,000 | 1.38% | ≈ 1 in 72 |
| Insertive anal sex | 11 per 10,000 | 0.11% | ≈ 1 in 909 |
These estimates assume exposure with someone who has detectable viral load and no prevention (no condoms, no PrEP, and no viral suppression on ART). Real-world risk can be far lower when prevention is used. Sources include the CDC risk tool methodology, NIH HIV information pages, and the per-act systematic review by Patel et al. (2014).
Most single exposures do not lead to transmission. HIV transmission is a chain of events, and chains often break. The purpose of these numbers is to rank exposures by biological efficiency and to guide prevention and testing decisions.
Anal vs vaginal: how baseline per-act estimates compare
Many people search for comparisons such as receptive anal versus insertive vaginal. The key point is that baseline estimates vary widely by tissue type and exposure mechanics. Below is a simple baseline comparison table using widely cited public health estimates.
| Exposure type | Per 10,000 exposures | Percentage | 1 in X |
|---|---|---|---|
| Receptive anal sex | 138 per 10,000 | 1.38% | ≈ 1 in 72 |
| Insertive anal sex | 11 per 10,000 | 0.11% | ≈ 1 in 909 |
| Receptive vaginal sex | 8 per 10,000 | 0.08% | ≈ 1 in 1,250 |
| Insertive vaginal sex | 4 per 10,000 | 0.04% | ≈ 1 in 2,500 |
All per-act estimates above are conditional on exposure with a partner who has transmissible HIV and no prevention used. Real-world conditions can be very different, especially with PrEP, condoms, and viral suppression (U=U).
Why anal sex has higher risk: the biology in plain language
For HIV to transmit sexually, four things generally have to line up:
- Enough virus in the source fluid — viral load is the main driver of this.
- Access to susceptible tissue — mucosa that is thin, inflamed, or micro-injured makes access easier.
- Presence of target cells — HIV preferentially infects activated CD4 T cells, especially those expressing CCR5.
- Time and contact — longer or repeated exposure increases probability, even if any single event is unlikely.
This is why viral suppression (U=U), PrEP, and condoms are so powerful. They break this checklist at multiple points.
Rectal lining structure is physically more vulnerable
The rectum is lined by a mucosal surface designed for absorption, not abrasion. In immunology terms, the rectal mucosa is often described as having a single layer of columnar epithelial cells, which can be more susceptible to mechanical disruption than thicker, multi-layered squamous epithelium found in other sites.
Friction can create microtrauma — tiny tears that are not visible, but can allow virus access past the surface barrier. Even without visible blood, microscopic disruption and inflammation can occur.
Discussed in mucosal immunology reviews and rectal mucosa studies, including Caputo et al. (2023).
The rectum is rich in HIV "target cells"
HIV preferentially targets activated CD4 T cells, especially those expressing the CCR5 co-receptor. Rectal tissue is part of the broader gut-associated immune system, and it contains many immune cells close to the surface.
Several lines of research show that rectal mucosa can have a distinctive immune phenotype in people engaging in condomless receptive anal intercourse, including inflammatory signatures and higher levels of relevant T-cell subsets.
See rectal mucosa phenotype work by Kelley et al. and mucosal transmission reviews.
Fluid exposure and contact time can be higher
Receptive exposure places infectious fluid in direct contact with a vulnerable mucosal surface. If semen is present, it can remain in contact with rectal tissue for a period of time, especially if there is no barrier method.
That combination — direct contact plus vulnerable tissue plus immune target cells — is a major reason receptive anal sex sits at the top of per-act risk rankings.
Inflammation and STIs increase susceptibility
Inflammation recruits activated immune cells to the tissue and can weaken barrier function. Many sexually transmitted infections have been consistently associated with increased HIV acquisition risk, though the size of the increase varies by organism and population.
Ulcerative conditions can increase vulnerability because they remove barrier layers entirely.
Reviews on STI-HIV synergy and mucosal inflammation discuss these pathways.
Receptive vs insertive: why the numbers diverge
"Receptive" and "insertive" describe which body surfaces are exposed to infectious fluid, and how vulnerable those surfaces are. The per-act estimates reflect that biology.
Highest baseline per-act estimate
A widely used estimate is 138 transmissions per 10,000 exposures, or 1.38% per act, in the absence of prevention and assuming the partner has detectable viral load.
If the partner is undetectable on ART, the expected sexual transmission risk collapses towards zero in large observational datasets.
Lower than receptive, but not zero
Insertive anal sex is commonly estimated at 11 transmissions per 10,000 exposures, or 0.11% per act — roughly 1 in 909, assuming detectable viral load and no prevention.
Insertive risk exists because infection can occur through microabrasions, the urethral opening, and for uncircumcised men, the inner foreskin, which is mucosal tissue containing HIV-susceptible immune cells.
Research on penile tissue immune cell distribution and foreskin biology helps explain why circumcision reduces female-to-male acquisition in some contexts.
- These numbers are conditional. They assume a partner with transmissible HIV and no prevention.
- Risk varies by orders of magnitude with viral load, especially in acute infection before diagnosis or treatment.
- Repeated exposures accumulate probability. Low per-act does not mean low over many acts.
- Population averages hide heterogeneity. People are not averages, but biology still ranks exposures by efficiency.
What changes risk the most (biggest effect sizes first)
If you want maximum scientific clarity, prioritise the variables with the largest effect size. These are the levers that consistently move risk the most in real life.
Viral suppression (U=U)
The strongest real-world risk reducer is an HIV-positive partner maintaining an undetectable viral load. Large studies of serodifferent couples reporting condomless sex observed no linked transmissions when viral load was undetectable.
Public health guidance supports U=U, and major cohort studies have published zero linked transmissions with sustained suppression.
PrEP
Consistent PrEP use dramatically reduces acquisition risk from sex. Major public health messaging commonly cites around a 99% reduction in sexual acquisition risk with correct adherence.
Adherence matters because drug levels at the exposure site are what provide protection.
Condoms
Condoms reduce exposure by acting as a physical barrier that prevents contact between infectious fluid and vulnerable tissue. Consistency and correct use matter because breaks and slippage change exposure.
From a mechanism standpoint, condoms reduce the chance the transmission checklist lines up.
Inflammation, trauma, and STIs
Inflammation increases susceptibility by recruiting activated immune target cells and altering barrier integrity. STIs can amplify inflammatory signalling and, in ulcerative cases, remove barrier layers entirely. Pain, irritation, or bleeding can indicate higher vulnerability.
This is one reason lube, gentle technique, and stopping if painful can matter in harm reduction terms.
Acute infection and very high viral load
Early HIV infection can involve extremely high viral load, which increases infectiousness. In population modelling and epidemiology, acute infection is often discussed as a period of elevated transmission probability compared to chronic infection.
"Unknown" status spans everything from undetectable to newly infected and untreated.
Insertive modifiers (foreskin, microtears)
Insertive risk can increase with irritation, abrasions, or inflammation. For uncircumcised men, the inner foreskin is mucosal tissue where HIV-susceptible immune cells may be positioned closer to the surface.
This does not mean circumcised equals immune. It means some barriers are stronger than others.
PEP and testing timeline (what to do after an exposure)
If an exposure is genuinely higher risk and recent, two decisions matter: whether PEP is appropriate, and when to test for reliable results. If anxiety is spiking, a clear plan beats symptom-scanning.
Time-sensitive, best started as soon as possible
PEP is an emergency intervention after potential HIV exposure. Guidance typically emphasises starting as soon as possible, and it is generally not recommended if started after 72 hours.
If you are within that window, seek urgent clinical advice. Do not wait for symptoms.
Match the test to the window period
A modern 4th generation lab test (antigen/antibody) can detect infection earlier than antibody-only tests. Testing too early can produce false reassurance and worsen anxiety.
For a deeper breakdown, see: HIV testing window periods.
Symptoms are not a reliable early signal for HIV. Risk assessment is primarily about exposure type, partner infectiousness (viral load), and prevention used. Build a testing plan and execute it.
Frequently asked questions
The baseline per-act estimate is highest when the partner has transmissible HIV and no prevention is used. If a partner is undetectable (U=U), or if PrEP and condoms are used correctly, the real-world risk can be dramatically lower.
Oral transmission is rare because the mouth and saliva are generally less favourable environments for HIV transmission, and intact oral tissues provide different barriers than rectal mucosa. Risk can increase with bleeding gums or sores, but overall per-act risk remains far lower than anal intercourse in public health estimates.
It can reduce exposure, but it does not eliminate risk because pre-ejaculate can be present, and microscopic blood can occur. Viral load, tissue condition, and prevention used usually matter more than a single detail.
Large studies of serodifferent couples reporting condomless sex observed no linked transmissions when the HIV-positive partner had undetectable viral load. Public health guidance uses this evidence to support U=U messaging.
Seek urgent advice about PEP. The benefit is time-sensitive and guidance emphasises starting as soon as possible.
Sources & references
- NIH HIVinfo — per-act risk estimates: hivinfo.nih.gov transmission facts
- CDC HIV Risk Reduction Tool — about the data: hivrisk.cdc.gov about the data
- CDC — About HIV (U=U): cdc.gov HIV about
- Patel P, et al. (2014) Systematic review of per-act HIV transmission risk: PubMed · Full text (PMC)
- Rodger AJ, et al. (2019) PARTNER study — zero linked transmissions with undetectable viral load: The Lancet
- Caputo V, et al. (2023) Mucosal structure and early HIV interplay: Frontiers in Immunology
- Kelley CF, et al. (2016) Rectal mucosa phenotype in MSM: Full text (PMC)
- Ward H, Rönn M. (2010) STI and HIV acquisition association review: Full text (PMC)
- Passmore JAS, et al. (2016) Genital inflammation and HIV acquisition biology: Full text (PMC)
- Miller WC, Rosenberg NE, et al. (2010) Acute and early infection contribution to transmission: Full text (PMC)
- Hollingsworth TD, Anderson RM, Fraser C. (2008) Transmission by stage of infection: PubMed
- McCoombe SG, Short RV. (2006) HIV target cells in penile tissues: PubMed
- Zhou Z, et al. (2011) Inner foreskin susceptibility mechanisms: PLOS Pathogens
This article is for education, not diagnosis or personal medical advice. If you believe you had a higher-risk exposure, or you are within a time window where PEP may apply, contact a clinician or sexual health service.