Can You Get HIV From Oral Sex?
🕓 Last updated: 02 May 2026
A calm, science-based guide to oral sex, HIV risk, testing, and when specific factors can change the picture.
HIV transmission from oral sex is considered extremely low risk in typical real-world scenarios.
Oral sex is considered low risk for HIV because the mouth has several natural protective barriers, and most oral exposures do not expose vulnerable tissue to enough virus to cause infection. Low risk does not mean zero risk, but the risk from oral sex is much lower than the risk from unprotected vaginal or anal sex.
The main things that change the picture are visible blood, open sores, major gum disease, ejaculation in the mouth, and a partner with a high viral load.
Most oral-only exposures are very low risk for HIV. The details that matter most are ejaculation, visible blood, sores, dental trauma, and whether the partner may have a high viral load.
Private, anonymous, and based on the exact details of your encounter.
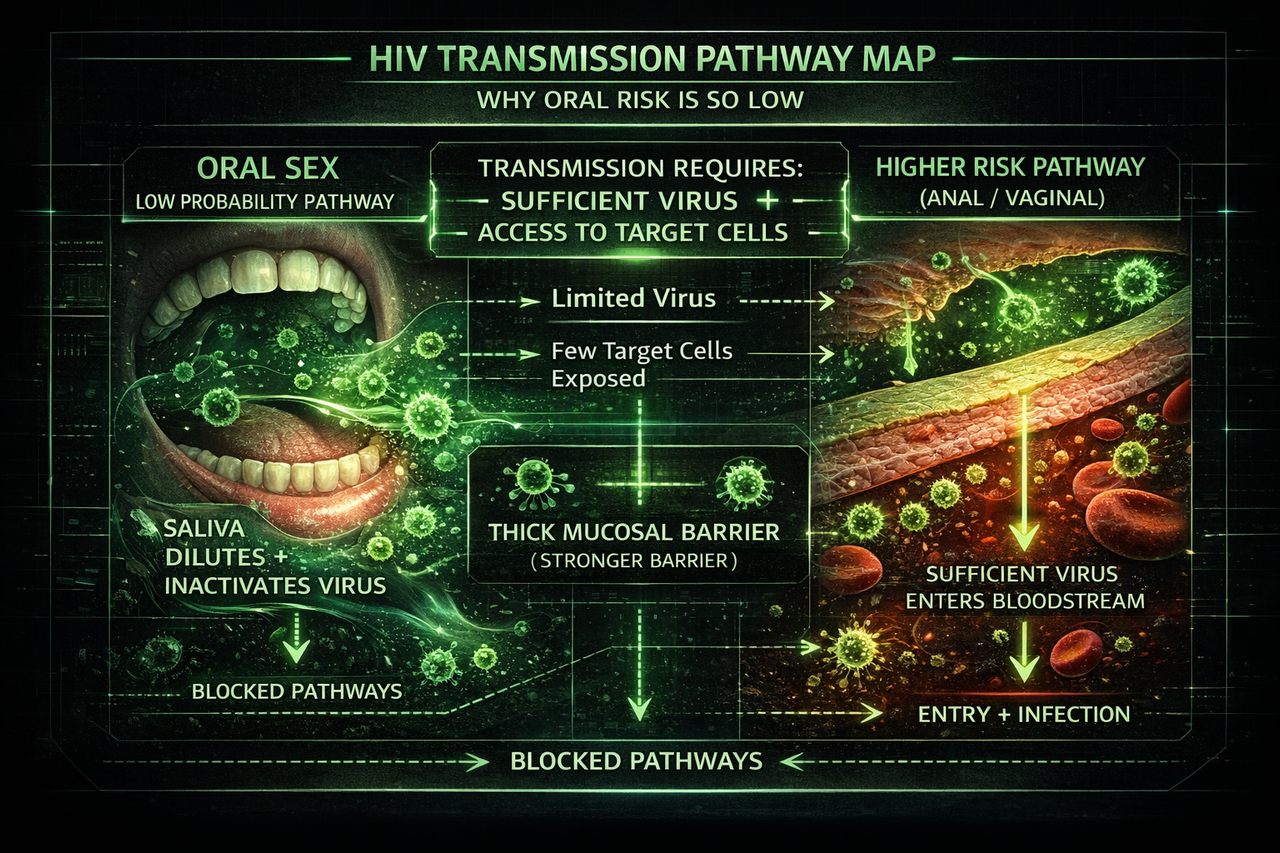
This visual shows why oral HIV transmission is considered extremely low risk. In most real-world scenarios, saliva reduces viral activity and intact mouth tissue limits access to target cells, meaning the conditions needed for infection are rarely met.
Can oral sex cause HIV?
Oral sex can transmit HIV in theory, but documented transmission is rare and the overall risk is considered much lower than unprotected vaginal or anal sex.
The risk is lowest when there is no visible blood, no open sores, no major gum disease, no ejaculation in the mouth, and no reason to believe the partner has a high viral load.
In plain language, most anxiety is about giving oral sex or putting your mouth on someone’s genitals. That direction has the higher theoretical risk because the mouth may contact semen, vaginal fluid, blood, or genital sores.
What is the HIV risk from giving oral sex?
Giving oral sex has the higher theoretical risk compared with receiving oral sex because the mouth may contact semen, vaginal fluid, blood, genital sores, or inflamed tissue. Even then, the risk is usually very low unless there is visible blood, open mouth sores, major gum disease, ejaculation in the mouth, or a partner with untreated HIV or a high viral load.
The most important question is not simply “did oral sex happen?” It is whether HIV had a realistic route into vulnerable tissue. Intact mouth tissue plus saliva makes transmission difficult. Bleeding gums, ulcers, recent dental work, or open sores make the theoretical pathway more relevant.
What is the HIV risk from receiving oral sex?
Receiving oral sex is generally considered extremely low risk for HIV in typical scenarios. Saliva is not an efficient HIV transmission fluid, and without blood or significant trauma, this route is not considered a major driver of HIV transmission.
Risk would only become more theoretically relevant if there was visible blood in the other person’s mouth, open sores, or significant trauma. In ordinary receiving-oral-sex scenarios, the risk is usually near the very bottom of the sexual-risk spectrum.
Does ejaculation in the mouth increase HIV risk?
Ejaculation in the mouth can increase theoretical HIV risk because it increases exposure to semen. The risk is still usually low, but it becomes more relevant if there are bleeding gums, mouth ulcers, recent dental work, sores, or a partner with untreated HIV or a high viral load.
If ejaculation happened but there was no blood, no sores, no mouth injury, and no reason to believe the partner has untreated HIV, the overall risk is still generally considered very low. The details matter, which is why a personalised risk review can be more useful than symptom-scanning.
Why HIV transmission through oral sex is so rare
For transmission to happen, HIV has to reach vulnerable cells in sufficient quantity. In the mouth, several defensive layers make that difficult. Think of it like a strong goal-line stand: multiple barriers have to fail for a score.
Saliva is not a friendly environment for HIV
Saliva contains enzymes and proteins that reduce viral activity, and it dilutes any virus that might be present. That combination makes it hard to maintain an infectious dose in typical oral exposure.
Mouth tissue is tougher than rectal tissue
The lining of the mouth is generally thicker and more resistant than the rectum. HIV has a harder time crossing intact oral tissue compared with thin, delicate mucosal tissue in other areas.
Typical exposure dose is lower
Most oral sex does not involve prolonged contact with a high concentration of infected fluid entering vulnerable tissue. Without blood, open sores, or heavy inflammation, the pathway into the bloodstream is usually not there.
Reality check: Oral sex is often described as “extremely low risk” because population-level data struggles to measure it as a meaningful driver of infections. That is not the same as impossible; it means the baseline probability is tiny in typical scenarios.
When the theoretical risk increases
Oral sex is not treated as zero risk in medical guidance because certain conditions can reduce the mouth’s natural barriers. Even then, the event usually remains low probability, but the logic is straightforward: more virus, more direct access, more vulnerability.
What pushes risk up
- Visible blood in the mouth or on genitals, especially heavy bleeding.
- Open cuts, sores, or ulcers in the mouth, including recent dental trauma.
- Severe gum disease with frequent bleeding and inflammation.
- Ejaculation in the mouth, which can increase exposure dose.
- High viral load in the partner, such as untreated HIV or acute infection.
What pushes risk down
- No blood, no sores, and no mouth injuries.
- No ejaculation in the mouth, or brief contact only.
- Effective ART with sustained viral suppression in the partner.
- Condoms or barriers used during oral sex.
- Lower partner likelihood based on realistic prevalence context.
“Extremely low” covers a lot of scenarios. The main swing factors are whether there was blood or open tissue, whether ejaculation happened, and whether viral load could plausibly be high. If you are within 72 hours and you think your exposure included blood, major mouth injury, or another higher-risk factor, read PEP and PrEP and speak with a clinician urgently.
Giving vs receiving oral sex
Direction matters because it changes who is exposed to fluid and where that fluid contacts vulnerable tissue.
Giving oral sex
This is where most HIV anxiety focuses. The mouth is the contact point, so the main theoretical risk is when virus meets open tissue, bleeding gums, or sores, especially with ejaculation in the mouth and high viral load.
Receiving oral sex
The person receiving oral sex is generally at extremely low risk in typical scenarios. Saliva is not an efficient HIV transmission fluid, and intact genital skin or mucosa usually does not create the same pathway seen in higher-risk exposures.
Bottom line: If there was no blood, no open sores, and no ejaculation in the mouth, most oral-only scenarios sit at the very low end of the risk spectrum.
Do you need an HIV test after oral sex?
For oral sex only, testing is often more about peace of mind than high statistical risk, especially if there was no blood, no sores, no major dental trauma, and no ejaculation in the mouth.
If you do test, use the correct window period. A lab-based 4th generation blood test is usually strongly reassuring from around 28 days and often considered conclusive around 45 days. At-home oral fluid antibody tests usually need longer, commonly up to 90 days.
If anxiety is driving the decision, testing can still be a rational way to end the loop. Just avoid testing too early and then spiralling because the result is not yet final.
What to do next if you are spiralling
Stop symptom chasing
Symptoms cannot confirm or rule out HIV. The fastest path to calm is a testing plan that matches the correct window period. Use this symptoms guide to stop feeding the spiral.
Use the right test at the right time
If you are unsure when results become reliable, use the window period guide so you do not test too early and spiral again.
Assess the actual exposure
Focus on what happened: giving or receiving oral sex, ejaculation, visible blood, sores, dental trauma, and partner status. Those details matter more than vague symptoms.
Note: This page is educational and not medical advice. If you believe you had a higher-risk exposure and you are within 72 hours, speak with a clinician urgently to discuss PEP.
Frequently asked questions
Can you get HIV from oral sex?
It is possible in theory, but in typical real-world scenarios it is considered extremely low risk. Most HIV infections are not caused by oral sex.
Is giving oral sex riskier than receiving it?
Yes. The person using their mouth has the higher theoretical risk, mainly when there is blood, open sores, bleeding gums, or ejaculation in the mouth with a partner who has a high viral load.
Do I need PEP after oral sex only?
In most guidance, oral-only exposure without blood, major trauma, or other high-risk features is not usually a scenario where PEP is recommended. If you are within 72 hours and worried about specific details, speak with a clinician urgently.
Should I test after oral sex?
If anxiety is high, testing can provide peace of mind even when statistical risk is very low. Follow standard HIV test window guidance so the timing matches the test type.
What matters most for oral sex risk?
The main drivers are whether there was blood or open tissue, whether ejaculation occurred in the mouth, and whether viral load could plausibly be high. Those factors are why “extremely low” can still vary between scenarios.
Can saliva transmit HIV?
Saliva is not considered an efficient HIV transmission fluid. In typical oral sex scenarios, saliva tends to dilute virus and contains substances that reduce viral activity.
General articles can explain the pattern, but your specific risk depends on the exact details: whether you gave or received oral sex, whether ejaculation happened, whether there was blood or sores, and whether the partner’s HIV status or viral load is known.
Private, anonymous, and built around the exact details of your encounter.
Sources & References
- NAM aidsmap, Oral sex and the risk of HIV transmission: https://www.aidsmap.com/about-hiv/oral-sex-and-risk-hiv-transmission
- CDC, HIV Risk and Prevention: https://www.cdc.gov/hiv/risk/index.html
- CDC, How HIV Spreads: https://www.cdc.gov/hiv/causes/index.html
- HIV.gov, How HIV Is Transmitted: https://www.hiv.gov/hiv-basics/overview/about-hiv-and-aids/how-is-hiv-transmitted
This article is for education only and does not diagnose HIV or replace medical advice. If you think you had a recent higher-risk exposure, contact a sexual health clinic or healthcare professional for personalised guidance.