Female-to-Male HIV Transmission Rate: Risk, Odds, and Why It’s Usually Lower
🕓 Last updated: 4 May 2026
A calm, evidence-based guide to female-to-male HIV transmission risk, including the estimated rate, why insertive vaginal exposure is usually lower risk than receptive vaginal exposure, and what actually changes the odds. If you are symptom-checking, read HIV symptoms: separating fact from fear, then use HIV test window periods to time your testing properly. If you want to see how we translate your details into a number, read the HIV risk calculator guide.
The estimated female-to-male HIV transmission rate from vaginal sex is about 4 per 10,000 exposures when the female partner has HIV and is not virally suppressed.
That equals about 0.04% per act, or roughly 1 in 2,500, before adjusting for factors like viral load, condom use, PrEP, circumcision, STIs, cuts, bleeding, or whether the partner is undetectable. Female-to-male transmission is possible, but it is generally less efficient than male-to-female vaginal transmission.
The number above is a broad per-act estimate, not your personal probability. Your actual risk depends most on whether the partner actually had HIV, whether they were on effective treatment, whether a condom was used, and whether there was genital inflammation, bleeding, or sores. If you want your exact scenario translated into a risk estimate and testing timeline, use the personalized HIV risk assessment.
What is the female-to-male HIV transmission rate?
The commonly cited estimated rate for female-to-male HIV transmission during vaginal sex is 4 transmissions per 10,000 exposures when the source partner has HIV and is not virally suppressed. As a percentage, that is 0.04% per act, or about 1 in 2,500.
Simple answer: yes, a man can get HIV from a woman through vaginal sex, but the average per-act risk is lower than the reverse direction. The estimate is about 0.04% per exposure for insertive vaginal sex, compared with about 0.08% per exposure for receptive vaginal sex.
This does not mean every encounter has the same risk. The estimate assumes the partner has HIV and does not account for major modifiers such as viral load, condom use, PrEP, circumcision, STIs, genital sores, bleeding, or whether the partner is undetectable.
Insertive vaginal sex
Estimated at about 4 per 10,000 exposures, or 0.04%, when the female partner has HIV and is not virally suppressed.
Receptive vaginal sex
Estimated at about 8 per 10,000 exposures, or 0.08%, when the male partner has HIV and is not virally suppressed.
Can a female transmit HIV to a male?
Yes. HIV can be transmitted from a woman to a man during vaginal sex if the woman has HIV and has enough virus in vaginal fluid or blood to create an exposure. The virus can enter through the urethral opening, the inner foreskin in uncircumcised men, or through cuts, sores, inflammation, or irritated tissue on the penis.
However, female-to-male vaginal transmission is usually less efficient than male-to-female transmission because the penis has a smaller vulnerable entry area, much of the penile surface is tougher external skin, and fluid contact is often shorter than semen exposure inside the vagina.
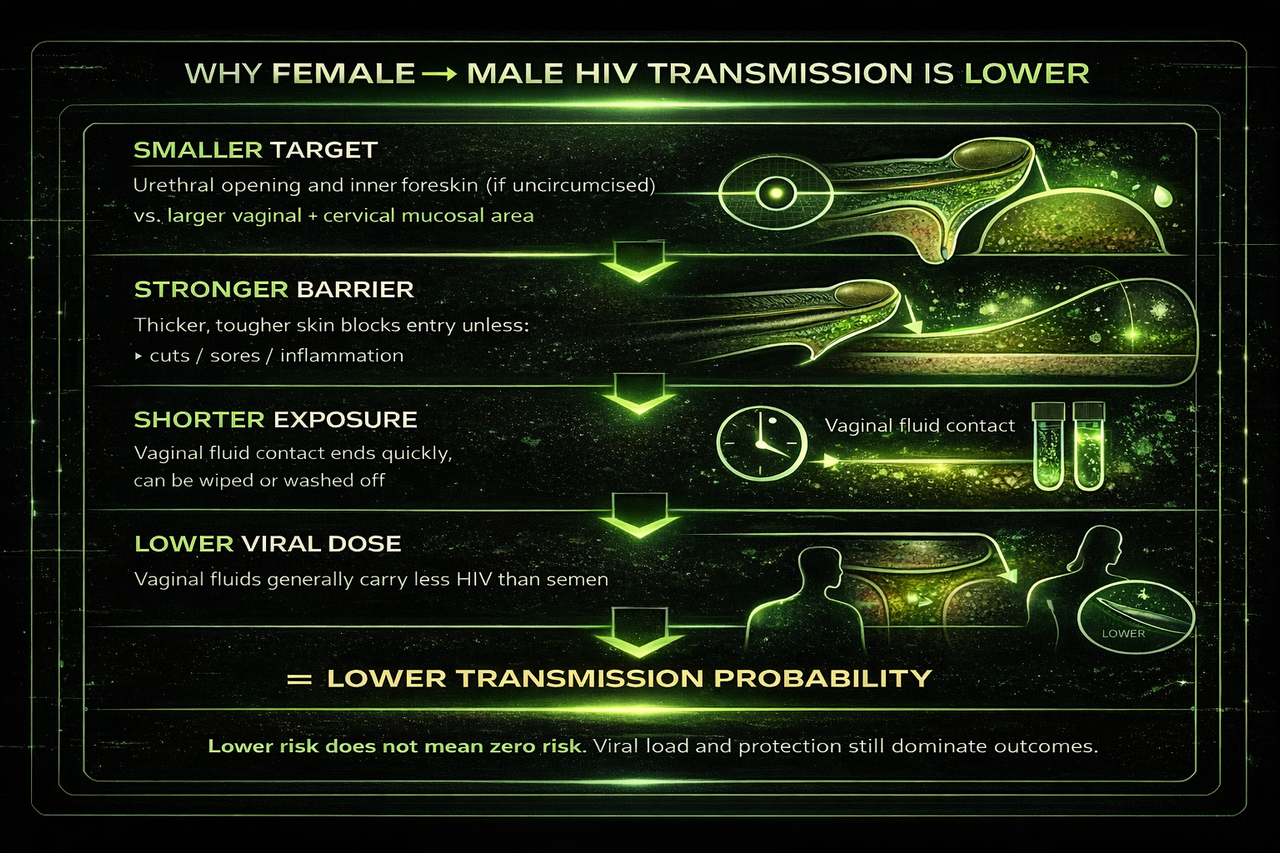
This visual summarises the main biological reasons female-to-male vaginal HIV transmission is usually less efficient: smaller vulnerable entry points, a stronger outer skin barrier, shorter average fluid exposure, and a lower average viral dose than the reverse direction. Lower risk does not mean zero risk, but it helps explain why this route is statistically less efficient.
If you are reading this, you are probably replaying the encounter and trying to guess your odds. That is normal. The goal here is to replace guessing with biology, realistic context, and a testing plan you can execute. If you are spiralling on signs or sensations, read HIV symptoms. If you want a clean timing plan, use HIV test window periods.
Why female-to-male transmission is generally harder
HIV transmission requires enough virus to reach vulnerable tissue and then cross into the bloodstream. In insertive vaginal sex, that path is usually harder for three core reasons.
Smaller vulnerable tissue area
The main entry points are limited. In men, the most vulnerable areas are the urethral opening and, if uncircumcised, the inner foreskin. Compared with the vagina and cervix, that is a smaller target.
Tougher outer barrier
Much of the penile surface is skin with a thicker protective layer. Skin is generally a stronger barrier than mucosal tissue, which makes it harder for the virus to cross unless there are cuts, sores, bleeding, or inflammation.
Shorter contact time and lower dose
Vaginal fluid exposure on the penis is often brief compared with semen exposure inside the vagina. In addition, average exposure dose can be lower in this direction, although viral load is still the biggest factor.
Key takeaway: Female-to-male HIV transmission is usually lower risk because there is less vulnerable surface area, a stronger external barrier, and often shorter and lower-dose exposure. Lower risk does not mean no risk.
Why women are more vulnerable in vaginal sex
In receptive vaginal sex, the biology is different. There is more vulnerable tissue, and exposure conditions usually favour longer contact. That is why male-to-female transmission is statistically more efficient on average.
Larger mucosal surface area
The vagina and cervix have a larger area of mucosal tissue, which contains immune cells that HIV can target. More surface area increases the chance of viral contact with susceptible cells.
Longer exposure time
Semen can remain inside the vaginal canal for hours, increasing contact time with mucosal tissue. Longer contact time generally increases opportunity for transmission when virus is present.
Micro-tears and inflammation matter more
Friction can cause tiny tears or irritation that are not visible. Inflammation from STIs can also increase vulnerability. These effects can be more meaningful when exposure is internal and prolonged.
Key takeaway: Women are more vulnerable in vaginal sex because exposure is internal, longer-lasting, and involves more mucosal tissue that can be susceptible to infection.
What actually changes female-to-male HIV risk?
The direction of sex matters, but the biggest swing factor is usually viral load. Risk rises most when the partner is untreated, newly infected, or has a high viral load, and it drops sharply when effective treatment suppresses the virus. If you are within 72 hours and you believe your exposure was higher-risk, read PEP after possible HIV exposure and speak with a clinician urgently.
Higher-risk conditions
Common factors that can increase transmission probability include:
- High viral load, especially during acute infection or untreated HIV
- No condom, or condom breakage or slippage
- STIs or inflammation in either partner
- Cuts, sores, bleeding, or irritation on the penis or vaginal tissue
- Menstruation or visible blood exposure if the partner has HIV and is not virally suppressed
- Uncircumcised penis, because the inner foreskin can be more vulnerable tissue
Protective factors
These are some of the strongest risk reducers:
- Effective ART with sustained viral suppression
- Condom used correctly and stayed intact throughout
- PrEP for the HIV-negative partner, when taken correctly
- Circumcision, which can reduce male acquisition risk in heterosexual exposure
- Lower partner likelihood based on realistic local prevalence and known testing history
When is female-to-male HIV risk higher?
Female-to-male risk is usually lower on average, but it can rise when the exposure involves a higher viral dose or an easier entry route. The biggest risk factor is a high or unknown viral load in the partner with HIV.
- Known HIV-positive partner not on treatment: risk is higher than if the partner is undetectable.
- Acute HIV infection: viral load can be very high early after infection.
- No condom or condom breakage: more direct fluid contact occurs.
- Uncircumcised penis: the inner foreskin can be more vulnerable tissue.
- STIs, sores, cuts, or inflammation: these can make tissue easier for HIV to cross.
- Menstruation or blood exposure: blood can increase exposure concern if the partner has HIV and is not suppressed.
General articles cannot combine partner likelihood, treatment context, condom use, inflammation, circumcision, PrEP, and exposure role into one probability for your exact encounter. If you want a personalised female-to-male HIV risk estimate plus a testing timeline with exact dates, use the risk assessment. If you want to see the logic behind the estimate, read the HIV risk calculator guide.
Frequently asked questions
Can a man get HIV from a woman through vaginal sex?
Yes. The average probability is lower than the reverse direction, but it is not zero. Risk is most influenced by viral load, condom use, inflammation or STIs, cuts or sores, circumcision status, and whether effective treatment is suppressing the virus. If you want a single personalised probability, use the assessment.
What is the female-to-male HIV transmission rate?
The commonly cited estimate for insertive vaginal sex is about 4 transmissions per 10,000 exposures, or 0.04% per act, when the female partner has HIV and is not virally suppressed. This is a broad average, not a personalised estimate.
What are the odds of getting HIV from a woman?
If the woman has HIV and is not virally suppressed, the broad estimate for insertive vaginal sex is about 4 per 10,000 exposures, or 0.04% per act. Your real-world odds may be much lower if her HIV status is unknown, local prevalence is low, a condom was used, she is on effective treatment, or you take PrEP.
Is female-to-male HIV transmission common?
It is possible, but it is not one of the most efficient sexual transmission routes. Female-to-male vaginal transmission is estimated to be lower than male-to-female vaginal transmission and much lower than receptive anal sex.
Why is female-to-male transmission less efficient?
The penis has a smaller area of vulnerable mucosal tissue, much of the surface is a stronger skin barrier, and exposure can be shorter. In many cases, the exposure dose can also be lower than semen exposure inside the vagina.
Does circumcision reduce a man’s HIV risk?
It can. The inner foreskin is a more vulnerable tissue, and circumcision reduces that exposure surface. It does not make risk zero, but it can lower average acquisition probability in heterosexual exposure.
Does menstruation increase female-to-male HIV risk?
Menstruation can increase concern because blood can contain HIV if the partner has HIV and is not virally suppressed. The actual risk still depends on viral load, condom use, visible blood exposure, sores, inflammation, and whether the partner is on effective treatment.
If we used a condom, is female-to-male risk basically gone?
Condoms dramatically reduce risk when used correctly and they do not break or slip. If anxiety is still high, testing at the correct window provides the cleanest reassurance. Use HIV test window periods so you do not test too early.
If my partner is on treatment and undetectable, what does that mean?
Sustained viral suppression on effective ART greatly reduces sexual transmission risk. If you are unsure about treatment consistency or timing, a standard testing plan can provide peace of mind. If you are within 72 hours and worried, read PEP and PrEP.
What testing window should I follow?
Test timing depends on test type. A simple framework:
- 4th generation blood test: reliable around 28 days, often treated as conclusive by 45 days in many guidelines.
- RNA/PCR test: can detect earlier in some cases, but usually needs a follow-up 4th generation test later.
- Oral swab antibody tests: longer window, often treated as conclusive at 90 days.
For a full explanation, see the window period guide. If symptoms are what is driving the spiral, read HIV symptoms.
Should I consider PEP after vaginal sex?
PEP is time-sensitive and is typically discussed when exposure is higher-risk and within 72 hours. If you are within that window and worried, seek urgent clinical advice quickly. Start here: PEP and PrEP.
Can symptoms confirm anything here?
No. Symptoms overlap with many common infections and anxiety. HIV status is determined by testing at the right time, not symptom scanning. If you are stuck in symptom interpretation, read HIV symptoms.