PEP vs PrEP: What’s the Difference and Which One Do You Need?
🕓 Last updated: 03 May 2026
PEP is emergency medication after a possible HIV exposure. PrEP is prevention before exposure. This guide explains the difference, timing, who may need PEP, and when testing still matters.
If a possible HIV exposure happened within the last 72 hours, do not wait. Contact a sexual health clinic, emergency department, urgent care provider, or doctor as soon as possible to ask about PEP. PEP works best the sooner it is started and is not usually started after 72 hours.
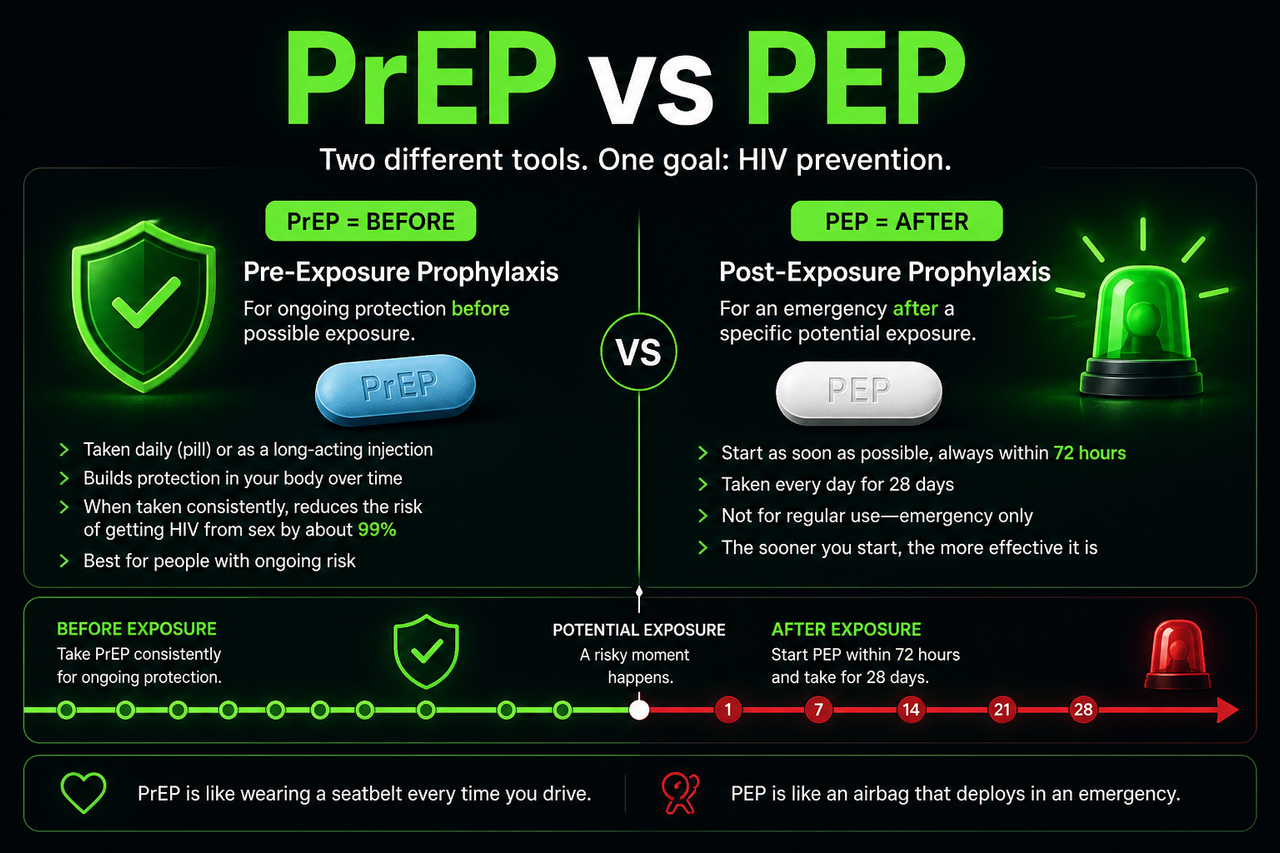
PrEP is before exposure. PEP is after exposure.
PrEP is used by HIV-negative people who want ongoing protection before sex or injection-related exposure. When taken as prescribed, PrEP is highly effective at preventing HIV from sex.
PEP is a 28-day course of HIV medication used after a possible exposure. It is an emergency option and needs to be started as soon as possible, within 72 hours.
PrEP is like having the protection built into the game plan. PEP is the emergency two-minute drill after something went wrong. They are both important, but they are used at different times.
PrEP is before exposure. PEP is after exposure.
This visual shows the key difference: PrEP is planned protection before possible HIV exposure, while PEP is an emergency 28-day course started as soon as possible after a specific exposure, within 72 hours.
PEP vs PrEP: the simplest difference
PEP and PrEP sound similar, but they solve different problems. PrEP, or pre-exposure prophylaxis, is taken before possible HIV exposure to prevent infection. PEP, or post-exposure prophylaxis, is taken after a possible exposure as an emergency measure.
Before exposure
PrEP is for people who are HIV negative and may have ongoing or repeated chances of being exposed to HIV. It can be taken as pills or long-acting injections depending on what is available and appropriate.
- Used before exposure.
- Designed for ongoing prevention.
- Requires HIV testing before and during use.
- Works best when taken as prescribed.
After exposure
PEP is for emergency situations after a specific possible HIV exposure. It is not a replacement for PrEP or condoms, and it is not meant to be used as a regular prevention plan.
- Used after a possible exposure.
- Emergency option only.
- Must be started within 72 hours.
- Taken every day for 28 days.
What is PrEP?
PrEP stands for pre-exposure prophylaxis. It is medication used by people who are HIV negative to reduce their chance of getting HIV before exposure happens. PrEP may be a good option for people with ongoing risk, such as sex with partners whose HIV status is unknown, partners who may have untreated HIV, or repeated situations where condoms may not be used.
PrEP can provide a steady prevention layer, but it is not something to start casually without testing and medical guidance. A clinician will usually confirm that you are HIV negative, check kidney function for some PrEP options, screen for hepatitis and STIs where appropriate, and help choose the right regimen.
PrEP is not emergency treatment for an exposure that already happened. If you are worried about a specific event from the last 72 hours, the urgent question is usually whether PEP is appropriate.
What is PEP?
PEP stands for post-exposure prophylaxis. It is a short course of HIV medication taken after a possible exposure to reduce the chance that HIV takes hold in the body. PEP is usually taken for 28 days.
The most important part of PEP is timing. It should be started as soon as possible after a possible exposure and within 72 hours. After 72 hours, PEP is generally not expected to work, so the next step usually becomes an evidence-based testing plan instead.
Every hour matters with PEP. If you are inside the 72-hour window and think the exposure could be meaningful, contact a sexual health clinic, emergency department, urgent care provider, or doctor now. Do not spend the whole window symptom-searching.
Do I need PEP after a possible HIV exposure?
PEP decisions depend on the details. A clinician will consider what happened, whether there was a realistic HIV transmission route, the partner’s known or estimated HIV status, whether the partner is on treatment and undetectable, whether a condom broke, whether ejaculation occurred, whether there was blood, and how long ago the event happened.
PEP is more likely to be considered after higher-risk exposures, such as condomless receptive anal sex with a partner who may have untreated HIV, a condom break during higher-risk sex, needle sharing, or certain occupational exposures. It is less likely to be recommended for very low-risk situations, such as casual contact, kissing, touching, or oral-only exposure without blood or major trauma.
If you are within 72 hours, get a clinical opinion first. If you are outside 72 hours, focus on the correct HIV testing window instead of replaying symptoms. For testing timing, read HIV test window periods.
Can I take PrEP after exposure instead of PEP?
No. PrEP is designed to prevent HIV before exposure. It is not the same thing as PEP and should not be used as a do-it-yourself substitute after a possible exposure.
If the exposure already happened and you are inside the 72-hour window, ask a clinician about PEP. If you keep having exposures that make you wonder about PEP, that may be a sign that PrEP should become part of your ongoing prevention plan.
When should you start PrEP instead of relying on PEP?
If you find yourself repeatedly worried after sex, repeatedly needing emergency advice, or repeatedly having condomless sex with partners whose HIV status you do not know, PrEP may be a better long-term prevention strategy.
PEP is the emergency response. PrEP is the prevention system. If the same risk pattern keeps showing up, the better play is not to keep needing the emergency drive. It is to fix the base defense.
- You have ongoing sex with partners whose HIV status is unknown.
- You have condomless anal or vaginal sex and want added HIV protection.
- You have a partner with HIV who is not consistently undetectable.
- You have needed PEP more than once.
- You inject drugs or share injection equipment.
- A specific possible exposure happened within the last 72 hours.
- A condom broke during a higher-risk encounter.
- You had condomless anal or vaginal sex with a partner who may have untreated HIV.
- You shared needles or injection equipment.
- A clinician decides the exposure has enough risk to justify emergency treatment.
Testing still matters after PEP or while on PrEP
PEP and PrEP are prevention tools, not replacements for testing. People starting PEP usually need baseline HIV testing, follow-up testing, and sometimes additional tests for kidney function, liver function, hepatitis, STIs, or pregnancy depending on the situation and local guidance.
PrEP users also need regular HIV testing to confirm they remain HIV negative and to monitor health while using the medication. Testing is the scoreboard. It is what turns worry into clear information.
If you are trying to work out when a negative result becomes reliable, read the HIV window period guide. If you are stuck on symptoms, read HIV symptoms: separating fact from fear.
What if the partner is undetectable?
If a partner living with HIV is on effective treatment and has a sustained undetectable viral load, sexual HIV transmission risk is effectively zero. This is often summarised as U=U, meaning undetectable equals untransmittable.
That context can dramatically change whether PEP is needed. If you know your partner is undetectable, read U=U and viral load for a deeper explanation.
What if the exposure was oral sex?
Oral sex is usually very low risk for HIV, especially when there is no visible blood, no mouth sores, no major dental trauma, and no ejaculation in the mouth. PEP is not usually considered for most oral-only exposures, but a clinician should decide when unusual factors are present.
For a full breakdown, read Can you get HIV from oral sex?.
Moving from panic to a plan
Feeling anxious after a possible HIV exposure is common. The way out is not endless symptom-checking. The way out is a simple sequence: check whether you are inside the PEP window, get clinical advice if you might need PEP, make a testing plan, and then reduce future risk with condoms, PrEP, U=U knowledge, or partner testing.
If you are trying to understand whether your specific encounter was low risk, higher risk, or worth discussing with a clinician, our confidential assessment can give you a structured HIV risk estimate and testing timeline based on your exact details.
Get my confidential risk assessmentFrequently Asked Questions
PrEP is taken before exposure as ongoing HIV prevention. PEP is taken after a possible exposure as an emergency 28-day course. PrEP is prevention planning. PEP is emergency response.
PEP should be started as soon as possible and within 72 hours of a possible HIV exposure. The sooner you start, the better. If you are inside the window, contact a sexual health clinic, emergency department, urgent care provider, or doctor promptly.
No. PrEP is designed for prevention before exposure. If the exposure already happened and you are inside the 72-hour window, ask a clinician whether PEP is appropriate.
Yes. PEP reduces the chance of HIV taking hold, but follow-up testing is still needed to confirm the outcome. For timing, use HIV test window periods.
PEP is designed as an emergency option, not as a regular strategy. If you find that you are needing PEP often, that is usually a sign that PrEP may be a better long-term prevention plan.
PrEP is highly effective for HIV prevention when used as prescribed, but it does not protect against other sexually transmitted infections or pregnancy. Many people use PrEP and condoms together for broader protection.
The safest move is to speak to a doctor or sexual health clinic as soon as possible, especially if you are inside 72 hours. A personalised risk assessment can help organise the details, but it should not delay urgent clinical care if PEP may be needed.
In many cases, yes. People who needed PEP may benefit from PrEP if similar risks could happen again. A clinic can advise on testing and timing so protection continues safely.
Sources & References
- CDC, Preventing HIV with PEP: https://www.cdc.gov/hiv/prevention/pep.html
- CDC, Preventing HIV with PrEP: https://www.cdc.gov/hiv/prevention/prep.html
- CDC HIV Nexus, Clinical Guidance for PEP: https://www.cdc.gov/hivnexus/hcp/pep/index.html
- HIV.gov, Post-Exposure Prophylaxis: https://www.hiv.gov/hiv-basics/hiv-prevention/using-hiv-medication-to-reduce-risk/post-exposure-prophylaxis
- HIV.gov, Pre-Exposure Prophylaxis: https://www.hiv.gov/hiv-basics/hiv-prevention/using-hiv-medication-to-reduce-risk/pre-exposure-prophylaxis
- BHIVA, UK Guideline for the use of HIV Post-Exposure Prophylaxis: https://bhiva.org/file/6183b6aa93a4e/PEP-guidelines.pdf
This article is for education only and does not replace medical advice. If you think you may need PEP, especially within 72 hours of a possible exposure, contact a clinician, sexual health clinic, urgent care provider, or emergency department promptly.