When Is PEP Recommended for HIV? A 72-Hour Exposure Guide
A calm, guideline-based guide to when HIV PEP is usually recommended, when doctors consider it case by case, and when it is usually not needed.
PEP is usually considered only if a possible HIV exposure happened within the last 72 hours. The sooner it is started, the better.
It is most often recommended after higher-risk exposures such as condomless receptive anal sex, a condom break with a partner who has HIV and is not known to be virally suppressed, sharing injecting equipment, or sexual assault with possible HIV exposure.
PEP is usually not recommended after oral sex alone in routine scenarios, intact-skin contact, saliva exposure, non-blood body fluids, a source who is confirmed durably undetectable, or exposures more than 72 hours ago.
Realism check: if guidelines say PEP is “not recommended” or “generally not recommended” in your situation, that usually means doctors do not view the exposure as high enough risk to justify emergency HIV treatment.
Do I need PEP after this exposure?
The cleanest way to think about PEP is not “am I scared?” but “does this exposure fit the medical decision lane for urgent HIV prevention?” Doctors usually look at the clock, the act, the fluid, the tissue exposed, and what is known about the source.
PEP is more likely if...
- The exposure happened within 72 hours.
- There was condomless receptive anal sex.
- A condom broke during higher-risk sex.
- The source has HIV and is not known to be undetectable.
- Needles, syringes, or injecting equipment were shared.
- There was sexual assault with possible HIV exposure.
PEP is usually not recommended if...
- More than 72 hours have passed.
- The exposure was oral sex alone in a routine scenario.
- The contact was only saliva, sweat, urine, tears, or intact skin.
- The source is confirmed durably undetectable on treatment.
- You were taking PrEP correctly.
- There was no realistic route for HIV to enter the body.
Not sure if your exposure fits the PEP window? Generate a private report that breaks down your exposure, risk lane, and testing timeline.
Check My PEP RiskHow doctors usually decide whether PEP is worth giving
Doctors do not usually make PEP decisions from fear alone. They are looking for three things: timing, type of exposure, and what is known about the source. The CDC describes PEP as appropriate when an exposure within the last 72 hours presents a substantial risk for HIV transmission. BHIVA and BASHH use similar logic, but break scenarios into lanes such as recommended, consider, generally not recommended, and not recommended.
Timing
PEP works in a narrow window. It should be started as soon as possible, and major guidelines say it should not be started later than 72 hours after the exposure.
Exposure type
The key question is whether HIV could realistically reach a vulnerable site such as the rectum, vagina, mouth, eye, non-intact skin, or bloodstream.
Source context
If the source has HIV and is not durably suppressed, the risk lane is higher. If the source is confirmed undetectable, the decision changes dramatically.
When PEP is usually recommended, considered, or usually not recommended
This infographic summarises the three main decision lanes doctors use when thinking about PEP: timing, exposure type, and what is known about the source.
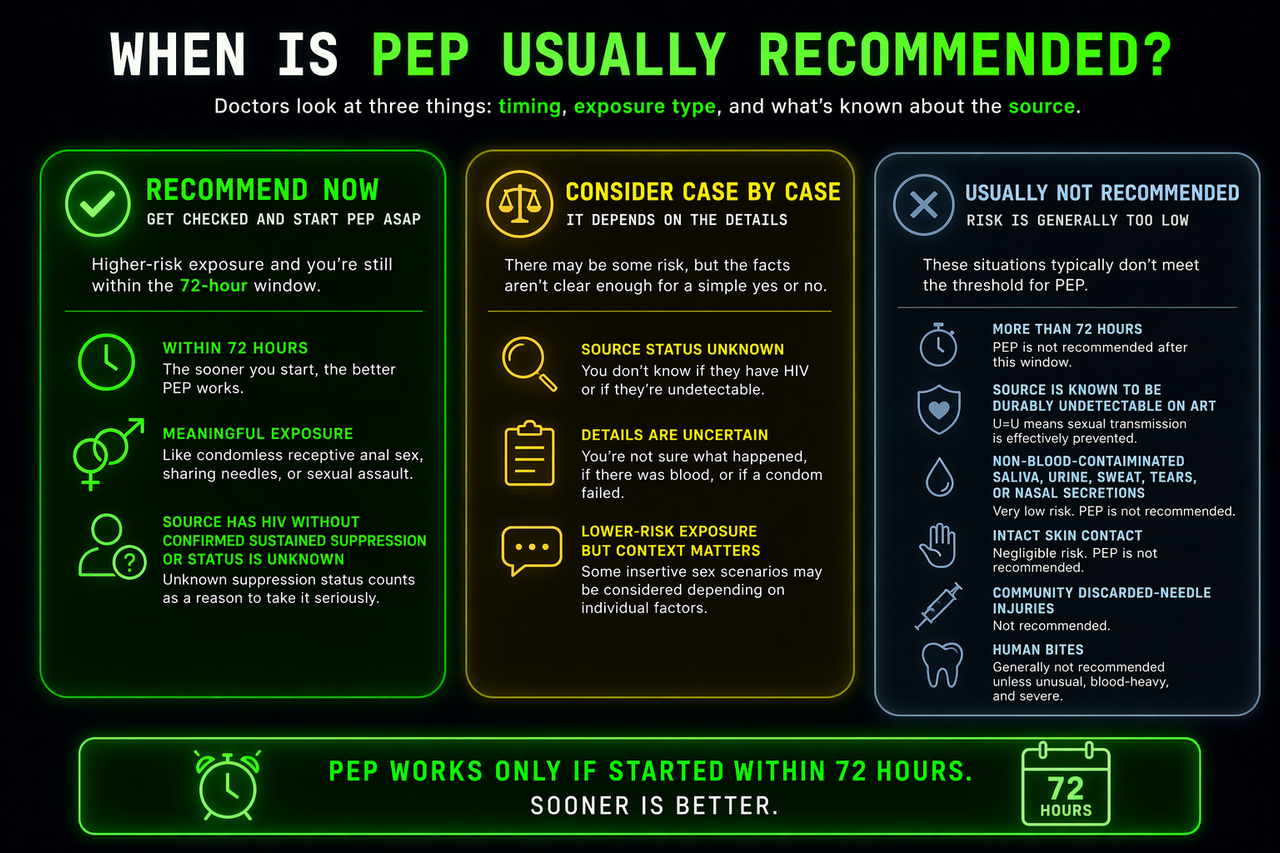
When PEP is usually recommended
These are situations where guidelines usually lean toward urgent action rather than reassurance. Exact recommendations vary by country and setting, but the following scenarios are the ones most likely to push doctors toward giving PEP quickly.
Condomless receptive anal sex within 72 hours
This is one of the clearest PEP scenarios in major guidelines, especially if the source is known to have HIV without confirmed sustained viral suppression, or if the source’s viral suppression status is unknown. Receptive anal exposure is treated seriously because rectal tissue is biologically vulnerable.
Sharing needles or injecting equipment
Sharing injecting equipment with a known HIV-positive partner who is not durably suppressed is a classic higher-risk PEP scenario. CDC public guidance also flags sharing needles, syringes, or other injecting equipment as a reason to seek urgent PEP assessment.
Sexual assault with possible HIV exposure
Sexual assault is an urgent-evaluation scenario because the details may be incomplete, tissue injury may be present, and the exposure can be high risk. This is exactly the kind of situation where the standard move is to seek immediate medical assessment rather than trying to calculate everything alone.
Blood or genital fluid to mucosa or non-intact skin
CDC guidance focuses on substantial-risk exposures to mucous membranes, non-intact skin, or the bloodstream. In other words, the issue is not just whether there was contact, it is whether the contact created a realistic path for transmission.
When PEP is sometimes considered, but not as automatically
Not every exposure lives in a clean yes-or-no lane. Some situations fall into a grey zone where the medical team may consider PEP case by case. This usually happens when there is some theoretical or low-level real risk, but the strength of the evidence is weaker or the exact facts are unclear.
Source status unknown
CDC says a case-by-case determination is needed when the exposure is substantial-risk but it is not known whether the source has HIV. That means unknown source status does not automatically mean “yes” and it does not automatically mean “no”. Doctors look at the act, the prevalence context, and any extra factors that raise or lower risk.
Some insertive exposures
BHIVA and BASHH place some insertive anal and vaginal exposures into a lower or more conditional lane than receptive anal sex. This is where clinicians often have to balance the biological route, the source context, and whether the exposure truly crosses the line into substantial risk.
When PEP is usually not recommended
This is the section that helps the most anxious readers. Many people panic after events that feel emotionally huge but do not actually fit the exposure patterns that doctors usually treat with PEP. These are the scenarios where guidelines often pump the brakes.
| Scenario | Why PEP is usually not recommended |
|---|---|
| More than 72 hours later | PEP is generally not recommended because it is unlikely to work once the recommended window has closed. |
| Source known to be undetectable on ART | If the source is durably undetectable and adherent, sexual transmission is effectively prevented, so PEP is usually not recommended. |
| Oral sex alone in most routine scenarios | Oral sex causes enormous anxiety, but it is generally not treated as a standard PEP scenario in guideline tables. |
| Saliva, urine, sweat, tears, or nasal secretions | Non-blood-contaminated secretions are not considered meaningful HIV transmission fluids in routine scenarios. |
| Intact skin contact | HIV does not move through normal intact skin the way panic often imagines. |
| Community needlestick injuries | Discarded-needle incidents are frightening, but the practical and biological risk is generally too low for routine PEP. |
| Human bites | PEP is generally not recommended unless there is an unusual blood-heavy injury with deep tissue trauma and a source likely to have a high viral load. |
Why reading “PEP not recommended” can actually help you calm down
This is the emotional heart of the article. If you were stressed after a sexual event and then saw that guidelines did not usually recommend PEP in your scenario, that can be stabilising for a reason. It means your event was measured against the same medical framework clinics use, not against raw panic.
The risk was judged too low for emergency HIV medication to be standard
“Not recommended” does not mean doctors are saying your feelings are irrational. It means the likely benefit of PEP did not appear high enough to justify taking emergency treatment, side effects, monitoring, and the hassle of a 28-day regimen.
It does not replace testing or clinical judgement
It still matters whether the facts were understood correctly. If there is doubt about what happened, whether the source was truly undetectable, whether blood was involved, or whether the timing is still inside 72 hours, that is still worth urgent medical discussion.
What to do if you are worried
Check the clock first
If it has been under 72 hours since a potentially substantial-risk exposure, do not sit on it. Seek urgent assessment right away. If it has been more than 72 hours, PEP is usually off the table and the next move is testing and follow-up.
Audit the actual exposure
Ask what body fluid was involved, what tissue it contacted, whether there was penetration, whether a condom failed, and whether the source is known to have HIV or be undetectable. This matters far more than how alarming the event felt.
Do not overread low-risk scenarios
Oral sex, saliva fears, intact skin contact, and community needlestick panic create a lot of spirals online. Those are exactly the situations where guidelines can help because they show what doctors usually do and do not treat as worth PEP.
Use testing for certainty
PEP is an emergency prevention decision, not a diagnosis. If you are outside the PEP window or your scenario was not usually PEP-worthy, the disciplined move is to build a proper testing plan instead of scanning your body for clues.
If you want a structured breakdown of your specific exposure, the likely risk lane, and the right testing timing, you can generate a private report based on your exact inputs.
Get My Confidential Risk ReportKeep building the full picture
PEP is only one part of the decision. These related guides can help you understand testing windows, condom failure, PrEP, and exposure-specific risk.
Frequently Asked Questions
Usually no. Major guidelines say PEP should be started as soon as possible and no later than 72 hours after exposure. After that, the standard approach usually shifts toward testing and follow-up rather than starting PEP.
For sexual exposure, usually no. If the source is known to be durably undetectable on treatment with good adherence, BHIVA and BASHH say PEP is not recommended for sexual exposure.
Usually not. Oral sex can create a lot of anxiety, but it is generally not treated as a standard PEP scenario in guideline tables. That said, unusual details, such as major blood exposure or severe oral injury, should still be discussed with a clinician.
It means the exposure is not an automatic yes or automatic no. Doctors look at the act, the tissue exposed, the fluid involved, the source context, and any extra factors that may raise or lower real transmission risk.
Not necessarily zero. It usually means the risk was judged too low for emergency HIV medication to be the standard move. That is different from saying nothing happened at all. Testing is still how certainty is built.
CDC says people taking PrEP as prescribed typically do not need PEP after a possible exposure. If adherence was inconsistent or there is any doubt, that still deserves a clinician conversation.
It depends on the exposure type, timing, and source status. A condom break during higher-risk sex within 72 hours deserves urgent clinical assessment, especially if the source has HIV and is not confirmed undetectable.
Sources & References
- CDC HIV Nexus, Clinical Guidance for PEP: cdc.gov/hivnexus/hcp/pep
- CDC, Preventing HIV with PEP: cdc.gov/hiv/prevention/pep.html
- CDC MMWR 2025, Antiretroviral Postexposure Prophylaxis After Sexual, Injection Drug Use, or Other Nonoccupational Exposure to HIV: cdc.gov/mmwr/volumes/74/rr/rr7401a1.htm
- WHO, Guidelines for HIV post-exposure prophylaxis: who.int/publications/i/item/9789240095137
- BHIVA / BASHH, UK Guideline for the use of HIV Post-Exposure Prophylaxis: bhiva.org/file/6183b6aa93a4e/PEP-guidelines.pdf
This guideline is especially useful because it explicitly separates scenarios into recommended, consider, generally not recommended, and not recommended.
This article is for education, not diagnosis or personal medical advice. If you think you had a substantial-risk HIV exposure within the last 72 hours, contact a clinician, sexual health service, urgent care service, or emergency department immediately. This page is designed to explain how guidelines usually think, not to replace real-time medical assessment.