Can HIV Pass Through a Condom?
A calm, scientific guide to protected sex, intact condoms, condom breakage, condom slippage, PEP timing, and when HIV testing makes sense.
HIV does not pass through an intact latex or polyurethane condom during sex. If the condom stayed on, covered the penis properly, was used from the start of penetration, and did not visibly break or slip off, the encounter is usually very low risk for HIV.
The real question is not whether HIV can seep through a normal intact condom. The real question is whether there was actual condom failure: breakage, slippage, late application, early removal, incomplete coverage, or unprotected contact with semen, vaginal fluid, rectal fluid, or blood.
High-standards call: review the actual exposure, not the panic. If there was clear condom failure and you are within 72 hours, speak with a sexual health clinic or clinician urgently about whether PEP is appropriate.

Can HIV pass through an intact condom?
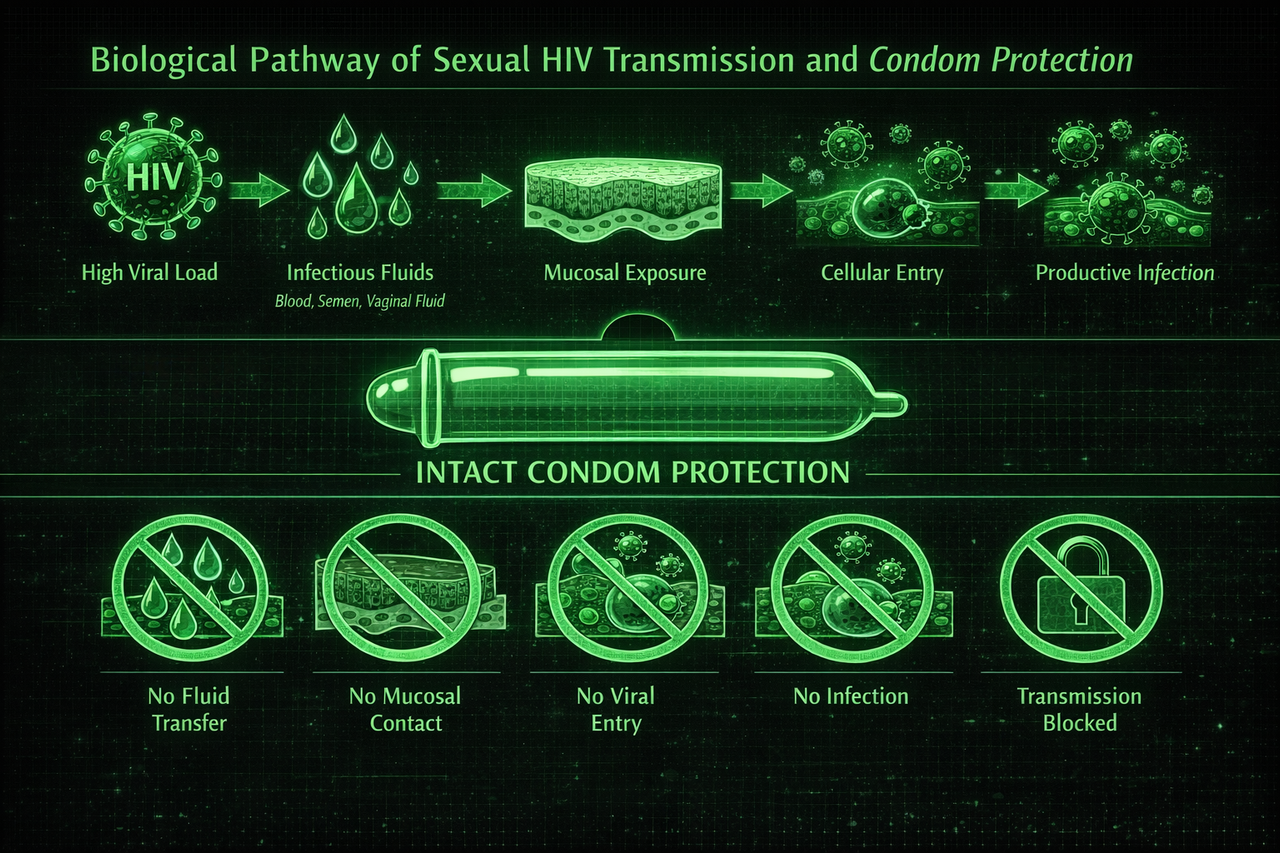
No, not in the way HIV anxiety often imagines. A normal intact latex or polyurethane condom is a physical barrier. It prevents direct exchange of semen, pre-ejaculate, vaginal fluid, rectal fluid, and blood with vulnerable mucosal tissue.
That is why public health guidance treats condoms as highly effective for HIV prevention when used correctly and consistently. The real-world risk comes from incorrect use or failure events, not from HIV magically moving through an intact barrier.
If the condom was on before penetration, stayed on the whole time, covered the penis properly, and did not break or slip off, HIV risk is usually very low. That does not mean condoms are mathematically perfect. It means the central exposure route was blocked.
How condoms protect against HIV
Condoms protect against HIV by interrupting the transmission pathway. HIV transmission requires an infectious fluid and access to vulnerable tissue. An intact condom blocks that contact during vaginal or anal sex.
What an intact condom does
- Blocks fluid exchange: semen and pre-ejaculate stay contained instead of reaching mucosal tissue.
- Reduces direct contact: the penis is separated from vaginal or rectal lining.
- Protects throughout sex: when used from the beginning and kept on throughout penetration.
- Changes the risk category: protected sex is assessed very differently from unprotected sex.
Why most protected encounters are lower concern
Many people with HIV anxiety focus on the fact that sex happened, then mentally downplay the condom. That is the wrong film review. If the condom stayed on and did its job, that is not a minor detail. It is the central protective factor.
What if the condom broke?
A broken condom changes the assessment because the barrier may no longer have blocked contact between fluids and vulnerable tissue. The level of concern depends on what kind of sex occurred, whether ejaculation happened, your role, the partner’s HIV status or viral load, and how long ago it happened.
If a condom clearly broke during vaginal or anal sex and you are within 72 hours, it is reasonable to seek urgent sexual health advice about whether PEP is appropriate. PEP is time-sensitive, so this is not the moment to lose hours symptom-scanning.
Inside 72 hours after a meaningful condom failure? Contact a sexual health clinic, urgent care provider, emergency department, or doctor promptly. A clinician can decide whether the exposure is significant enough for PEP.
What if the condom slipped off?
Condom slippage matters if it created unprotected penetration or fluid contact. A condom that shifted slightly but still covered the penis and stayed functional is different from a condom that came off inside the partner or was no longer protecting during penetration.
The key questions are: did penetration continue after the condom slipped, did the condom come off completely, was there ejaculation after it slipped, and was there direct genital-fluid contact with mucosal tissue?
Slippage without real exposure
The condom moved slightly but stayed on, still covered the penis, and there was no unprotected penetration. This is usually much less concerning.
Slippage with unprotected contact
The condom came off, penetration continued, or semen/genital fluids contacted vulnerable tissue. This should be assessed more like a possible exposure.
What if the condom was put on late or removed early?
A condom only protects the parts of sex where it was actually used. If penetration started before the condom was put on, or continued after it was removed, then there was some unprotected exposure.
The risk depends on the type of sex, duration of unprotected penetration, ejaculation, presence of blood or sores, and the partner’s HIV status or likelihood. Short unprotected contact is not the same as a full unprotected encounter, but it is also not the same as fully protected sex.
Does ejaculation change the risk if a condom was used?
If the condom stayed intact and semen remained inside it, ejaculation does not create the same HIV exposure as ejaculation without a condom. The condom’s job is to contain semen and prevent it from contacting vulnerable tissue.
Ejaculation becomes more relevant if the condom broke, slipped off, leaked because of obvious failure, was removed before ejaculation, or if semen spilled into contact with mucosal tissue after the condom came off.
What actually counts as condom failure?
If you are anxious, the brain starts treating any uncertainty as if it were proven failure. It is not. Risk assessment should separate clear failures from vague worries.
Events that genuinely matter
- Visible breakage or tearing: the condom split during sex or on withdrawal.
- Slipping off inside: the condom came off during penetration or remained inside the partner.
- Late application: penetration started before the condom was put on.
- Early removal: penetration continued after the condom was removed.
- Incomplete coverage: condom rolled only partway or kept bunching up.
Details that often trigger panic
- “I felt wetness”: lubricant, vaginal fluid, rectal fluid, or sweat can all be present even when the condom worked.
- “I did not inspect it perfectly”: not doing a lab-style check is not proof it failed.
- “It looked stretched”: stretching is normal and does not mean rupture by itself.
- “I am not 100% sure”: uncertainty is emotionally powerful, but it is not the same as known exposure.
People often feel moisture after sex and assume semen leaked through the condom. In reality, moisture can come from lubricant, the partner’s fluids on the outside of the condom, sweat, or normal genital secretions. Wetness alone is not reliable evidence that HIV exposure occurred.
Protected sex HIV risk: how to think about your encounter
The clean way to review the encounter is to separate three lanes: intact condom, definite failure, and uncertain-but-no-clear-failure. That keeps anxiety from calling every play a disaster.
Condom stayed intact
Used from the start, stayed on, covered properly, and did not break. This is usually very low concern for HIV.
Condom clearly failed
Broke, slipped off, was put on late, removed early, or left meaningful unprotected contact. This deserves a more careful exposure assessment.
No clear failure, just doubt
You are not fully certain, but you did not see breakage, slippage, or unprotected penetration. This is usually anxiety-driven uncertainty, not proof of exposure.
Do you need PEP after protected sex?
Usually, PEP is not the first concern if the condom stayed intact and was used correctly from start to finish. PEP becomes more relevant when there was a genuine exposure, such as condom breakage or slippage during higher-risk sex, especially if the partner may have untreated HIV or a high viral load.
PEP decisions should be made by a clinician and are time-sensitive. If you are within 72 hours and there was clear failure, seek urgent sexual health advice. If you are outside 72 hours, the focus usually shifts to correctly timed testing.
Do you need an HIV test after sex with a condom?
If the condom stayed intact and there was no meaningful failure, HIV testing may be more about peace of mind than high statistical risk. If the condom broke, slipped off, was put on late, or there was unprotected contact, testing can make sense based on the correct window period.
Do not test too early and then use a non-final result to keep the panic alive. A lab-based 4th generation blood test is usually strongly reassuring from around 28 days and often considered conclusive around 45 days. At-home oral fluid antibody tests usually need longer, commonly up to 90 days. For more detail, read HIV test window periods.
Protected sex with a sex worker: should you worry?
Protected sex with a sex worker often causes anxiety because people focus on partner category instead of the actual exposure route. The condom still matters. If the condom stayed intact, was used correctly, and did not break or slip off, the HIV risk is usually much lower than the fear suggests.
If the condom broke, slipped off, or there was unprotected anal or vaginal sex, then the assessment should focus on the specific act, role, partner likelihood, ejaculation, and timing. That is where a personalised risk estimate can be useful.
Protected sex with a known HIV-positive partner
If a partner is living with HIV, the most important question is whether they are on treatment and have a sustained undetectable viral load. If they are truly undetectable, sexual HIV transmission does not occur. This is known as U=U.
If viral load is unknown or the partner is not on treatment, an intact condom is still a major protective factor. If the condom failed and you are within 72 hours, speak with a clinician urgently about whether PEP is appropriate. For more context, read U=U and viral load.
What HIV anxiety gets wrong about condoms
HIV anxiety often refuses to accept protection because it wants absolute certainty. So it invents hidden failure modes: microscopic holes, invisible leaks, wetness as proof, or “maybe I missed something.”
“Can HIV molecules pass through microscopic holes?”
Public health guidance treats latex and polyurethane condoms as effective physical barriers for HIV prevention when used correctly. The practical concern is not invisible seepage through an intact condom. It is actual breakage, slippage, or incorrect use.
“What if there was a tiny leak and I missed it?”
Anxiety loves tiny hypothetical gaps. Risk assessment is not built on remote imagination. It is built on whether there was a real route of exposure.
What to do if you are panicking after sex with a condom
Review the facts
Did the condom stay on? Did it visibly break? Was it used before penetration began? Did penetration continue after it came off or was removed?
Check the 72-hour window
If there was genuine condom failure and the encounter could plausibly involve HIV exposure, urgent sexual health advice matters because PEP is time-sensitive.
Do not symptom-scan
Looking for fever, rash, throat pain, lymph nodes, or tongue changes will not settle the question. Exposure logic and testing windows are what matter.
Use the right test timing
If testing is needed, do it based on the correct window period, not panic. The right timing depends on the test type and when the encounter happened.
If you want a calm, evidence-based breakdown of your specific encounter, including whether the condom changed the risk picture and whether further action is warranted, you can generate a private report based on your exact details.
Get My Confidential Risk ReportRed flags: when to seek urgent help sooner
- The condom clearly broke or slipped off during vaginal or anal sex and you are within 72 hours.
- The partner is known HIV positive and not confirmed undetectable.
- There was unprotected receptive anal or vaginal exposure because those acts can carry higher concern.
- You are within the PEP window and cannot think clearly, because timely clinical advice beats losing hours to internet panic.
These are the situations where fast, disciplined action matters more than reassurance loops.
Frequently Asked Questions
In practical sexual health guidance, condoms are treated as effective physical barriers against HIV when used correctly and consistently. The main concern is not HIV passing through a normal intact condom, but whether the condom broke, slipped off, or was not used properly.
It is possible if the condom failed, slipped off, was put on late, removed early, or did not cover properly. If the condom stayed intact and was used from start to finish, the encounter is usually much lower concern for HIV.
A broken condom can create a possible exposure, especially during vaginal or anal sex. If this happened within 72 hours, seek urgent sexual health advice about whether PEP is appropriate.
Slippage matters if it caused unprotected penetration or fluid contact. A small shift while the condom still covered the penis is different from the condom coming off completely.
Wetness alone is not reliable evidence of condom failure. It can come from lubricant, vaginal fluid, rectal fluid, sweat, or other moisture outside the condom.
Usually the key issue is whether there was actual condom failure. If the condom stayed intact and on throughout sex, PEP is generally not the first concern. If it broke, slipped off, or there was other genuine exposure and you are within 72 hours, urgent sexual health advice makes sense.
If the condom stayed intact, testing may be more about peace of mind than high statistical risk. If the condom failed or unprotected contact occurred, testing based on the correct window period can make sense.
If a person with HIV is truly undetectable on treatment, sexual transmission does not occur. That is the meaning of U=U and it is one of the strongest protective facts in HIV prevention.
Sources & References
- CDC, Preventing HIV with Condoms: https://www.cdc.gov/hiv/prevention/condoms.html
- CDC, Condom Use Overview: https://www.cdc.gov/condom-use/index.html
- CDC, What Can Decrease HIV Risk: https://hivrisk.cdc.gov/can-decrease-hiv-risk/
- CDC, Preventing HIV with PEP: https://www.cdc.gov/hiv/prevention/pep.html
- HIV.gov, Preventing Sexual Transmission of HIV: https://www.hiv.gov/hiv-basics/hiv-prevention/reducing-sexual-risk/preventing-sexual-transmission-of-hiv
- WHO, Condoms Fact Sheet: https://www.who.int/news-room/fact-sheets/detail/condoms
- NHS, Condoms: https://www.nhs.uk/contraception/methods-of-contraception/condoms/
This article is for education, not diagnosis or personal medical advice. If a condom clearly broke or slipped off during a recent encounter, or you think there may have been genuine exposure and you are within 72 hours, contact a sexual health service or clinician urgently to discuss next steps.