How Does an Oral HIV Test Work?
A clear explanation of OraQuick, gum swab collection, HIV antibodies, test and control lines, accuracy, and why timing matters.
Oral HIV tests like OraQuick do not look for whole HIV virus in saliva.
They look for antibodies to HIV in oral fluid collected from the gums. Once that sample enters the device, it moves across a test strip. If HIV antibodies are present, they bind to HIV-related material fixed on the strip and create the test line. A separate control line appears to show the test ran properly.
That is why the mechanism matters. It is not a vague mouth swab. It is a specific antibody-binding reaction with a built-in control check.
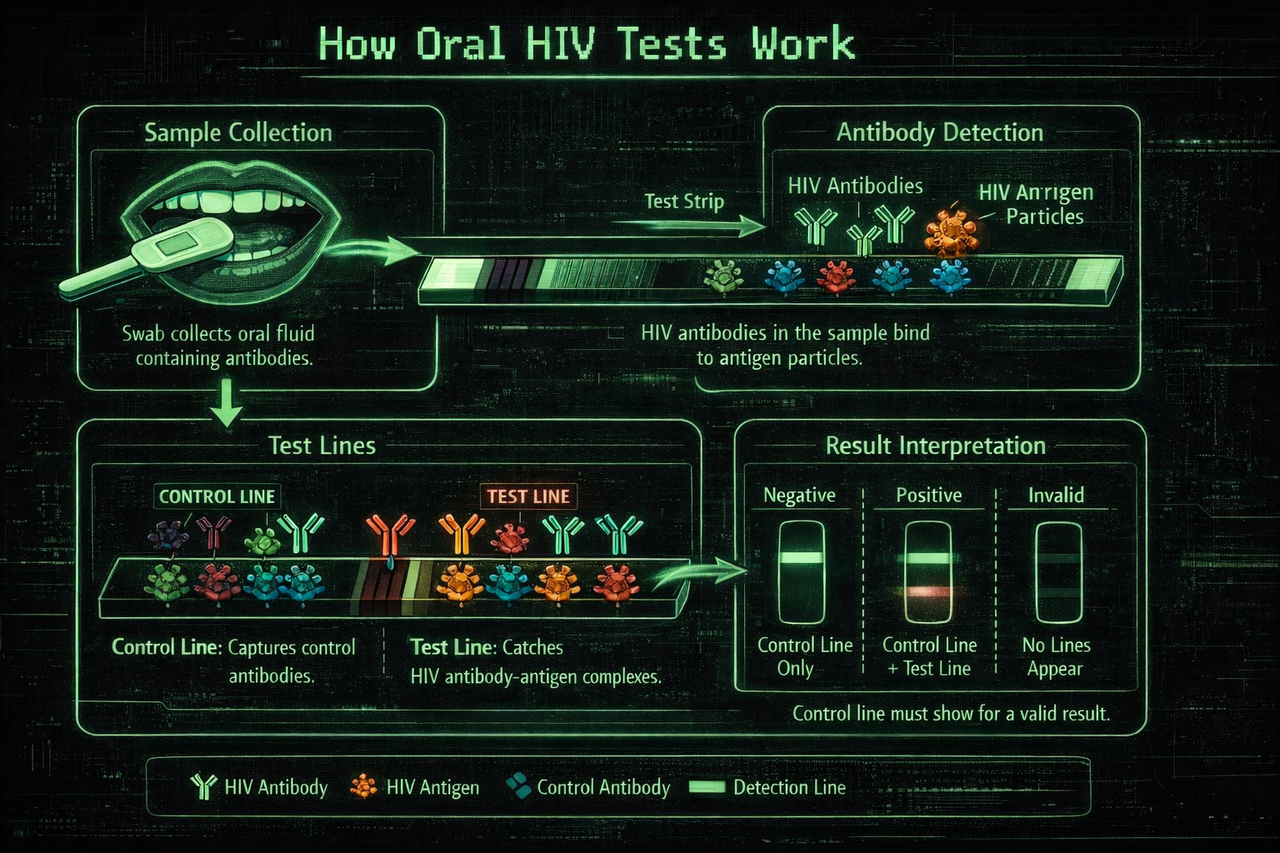
How the oral HIV test works
A visual breakdown of how the sample moves through the device, what triggers the control and test lines, and how the final result is read.
How accurate are oral HIV tests?
Oral HIV self-tests are designed to detect HIV antibodies in oral fluid. They can be useful and trustworthy when they are used correctly and enough time has passed after the possible exposure. They are not usually the best choice for ruling out a very recent exposure.
The main limitation is not that the test is random or mysterious. The main limitation is timing. OraQuick is an antibody test, so it depends on your body having had enough time to produce detectable antibodies. If you test too early, the result can be negative even if the immune response is still developing.
This is why many testing resources use a longer window for oral or rapid antibody tests than for laboratory 4th generation tests. A negative oral HIV test after the full window period is much easier to trust than a negative oral test taken soon after exposure.
The test can be reliable after the correct window period, but it is not designed to be the earliest possible HIV test. For recent exposure, a clinic or lab-based testing plan may be more appropriate.
Does OraQuick detect HIV in saliva?
No. OraQuick does not look for whole HIV virus floating in saliva. It is an oral fluid antibody test. The swab collects fluid from the gums, where HIV antibodies can be present after the body has had enough time to produce them.
That is why the instructions focus on swabbing the upper and lower gums, not the tongue, not the inside of the cheek, and not pooled spit.
What the test is actually looking for
A lot of people imagine an oral HIV test is trying to detect the virus itself in spit. That is not what it does.
OraQuick is an antibody test. It looks for the immune proteins your body makes in response to HIV. Those antibodies can be found not only in blood, but also in oral fluid collected along the gums. That is why the instructions tell you to swab the upper gum and lower gum, not the tongue, not the cheek, and not pooled saliva.
So the real question the test is asking is simple: are there HIV antibodies in this oral fluid sample?
Why the swab goes along the gums
This part matters more than most people realise. The test is designed to collect oral fluid from the gumline because that is where antibody-containing fluid can be picked up most reliably.
That is also why the instructions are so specific. One pass along the upper gum. One pass along the lower gum. Then the swab goes into the developer vial.
It is a controlled collection method, not random saliva sampling.
What actually causes the C and T lines to appear?
This is the part that helps most people relax. Once you understand the mechanism, the test stops feeling like a black box.
Inside the device is a test strip. The strip contains a nitrocellulose membrane, which is a material commonly used in rapid tests because fluid can move across it in a predictable way.
Fixed onto that membrane are synthetic HIV peptides. These act as the target material for HIV antibodies.
Test line
If HIV antibodies are present in the sample, they bind to the HIV-related material on the strip. That binding reaction produces a visible line in the test region, the T line.
Control line
A separate part of the strip, the control region, produces the C line. This line shows the sample and developer moved through the strip the way they were supposed to.
No HIV antibodies, no T line.
HIV antibodies present, T line appears.
Proper flow through the device, C line appears.
No C line, the test is invalid.
Oral HIV test result meanings
Reading the result is simple, but the timing of the test still matters. The C line tells you whether the test ran properly. The T line is the HIV antibody signal.
| Result | What it means | Next step |
|---|---|---|
| C line only | The test ran properly and no HIV antibody signal was detected. | If the exposure was within the last 3 months, test again after the window period or use a lab-based test plan. |
| C line and T line | The result is reactive, meaning the test detected an HIV antibody signal. | Get confirmatory testing from a clinic or healthcare provider. A self-test reactive result is not the final diagnosis by itself. |
| No C line | The test is invalid because the device did not run properly. | Repeat with a new test kit or seek testing from a clinic. |
| Faint T line | A visible T line, even if faint, should be treated as reactive. | Do not try to grade the line by darkness. Arrange confirmatory testing. |
How the device works from start to finish
Collect
The flat pad picks up oral fluid from the gums.
Develop
The stick goes into the developer vial, and the fluid begins moving through the strip.
React
If HIV antibodies are present, they bind at the test zone and trigger the T line.
Confirm
The control chemistry confirms the strip ran properly by producing the C line.
What materials are inside the test?
Part of what makes the device feel more trustworthy is knowing it is built from standard diagnostic materials, not vague mystery chemistry.
Nitrocellulose membrane
This is the surface the reaction happens on. It allows the sample to move steadily across the strip.
Synthetic HIV peptides
These are fixed in the test area. Their job is to capture HIV antibodies if they are present.
Anti-human IgG chemistry
This helps create the control line and shows the assay ran properly.
Developer solution
The vial contains a buffered solution that helps carry the sample through the strip.
The collection pad is the part you swipe along the gums to pick up the oral fluid sample.
Why understanding the mechanism can make the result easier to trust
A lot of HIV anxiety comes from not knowing what the test is actually doing. If the device feels mysterious, every result can start to feel fragile.
But the mechanism is not flimsy. A positive line does not appear out of nowhere. It appears because something in the sample bound to the HIV-related material on the strip strongly enough to create a visible signal. A valid test also has a control line to show the device actually ran.
That does not mean false results are impossible. No medical test works like that. But it does mean the result is not random. It is being produced by a specific reaction on a specifically designed strip.
OraQuick is not a vague saliva gadget making guesses. It is a small antibody test strip with a control system built in.
Why the main limitation is timing, not the basic mechanism
The biggest weakness of an oral HIV test is usually not poor chemistry. It is timing.
OraQuick is an antibody test. That means it depends on your body having had enough time to produce detectable antibodies. If someone tests too early, the result can be negative simply because the immune response is not far enough along yet.
So when people say oral HIV tests are “less accurate”, what they often really mean is that they are slower for early infection than some blood-based tests.
Once enough time has passed, the mechanism is straightforward and the test becomes much easier to trust.
Oral HIV tests are most limited by the window period. Use the free HIV window period calculator to see whether your test timing is too early, reliable, or conclusive.
Use The HIV Window Period CalculatorIf you are stuck second-guessing your exposure, test timing, or result, get a personalised report built around your exact situation.
Run AssessmentFrequently Asked Questions
An oral HIV test collects oral fluid from the gums and checks for HIV antibodies. If antibodies are present, they bind to HIV-related material on the test strip and create the T line. The C line shows the test ran properly.
Not in the way most people think. It detects HIV antibodies in oral fluid collected from the gums, not whole HIV virus floating in spit.
Oral HIV tests can be trustworthy when used correctly and after the full window period. Their main limitation is that they are antibody tests, so they are not the best option for detecting very recent infection.
The T line appears when HIV antibodies in the sample bind to the HIV-related material fixed on the strip.
The control line appears when the test runs properly and the sample flows through the device as intended.
It means the test is invalid. The device did not run properly, so the result cannot be trusted.
A visible T line, even if faint, should be treated as reactive. Do not try to judge the result by line darkness. Arrange confirmatory testing with a clinic or healthcare provider.
Usually because they do not understand what the test is detecting. Once you realise it is an antibody-binding test with a control line, it feels much less vague.
Timing. If someone tests too early, before enough antibodies have developed, the test can miss a recent infection.
Sources & References
- FDA, Information regarding the OraQuick In-Home HIV Test: https://www.fda.gov/vaccines-blood-biologics/approved-blood-products/information-regarding-oraquick-home-hiv-test
- OraQuick UK, Instructions for Use: https://uk.oraquick.com/media/howtouse/instructions/3/0/3001-3224_rev_0324_oraquick_self-test_ifu_uk_english.pdf
- OraQuick Global, Instructions for Use: https://global.oraquick.com/media/howtouse/instructions/3/0/3001-3031-OQ_Self_Test-ENG.pdf
- FDA, OraQuick ADVANCE Rapid HIV-1/2 Antibody Test package insert: https://www.fda.gov/media/73607/download
- CDC, Self Testing: https://www.cdc.gov/stophivtogether/hiv-testing/self-testing.html
- CDC, HIV Testing: https://www.cdc.gov/hiv/testing/index.html
This article is for education only, not diagnosis or personal medical advice. A reactive self-test still needs confirmatory testing. A negative oral antibody test does not rule out very recent infection.