HIV and Fingernails: Can HIV Cause Nail Changes, or Is Anxiety Filling in the Gaps?
A calm, scientific guide to fingernail changes, what HIV does and does not usually do, and why exposure plus testing beats symptom-scanning.
Fingernail changes are not a classic early sign of acute HIV. When people first acquire HIV, the symptoms that get discussed most often are flu-like symptoms such as fever, rash, sore throat, swollen glands, fatigue, and muscle aches, not a sudden distinctive fingernail pattern.
Can HIV affect nails at all? Yes, but usually in a more indirect way. Nail problems in people living with HIV are generally non-specific and more often linked to fungal infection, medication effects, or more advanced immune suppression rather than a unique “HIV nail” look.
Realism check: if your fingernails changed and your anxiety spiked, that reaction is understandable. But the high-standards call is this, nails are weak evidence for HIV. Exposure details and correctly timed testing carry the ball.
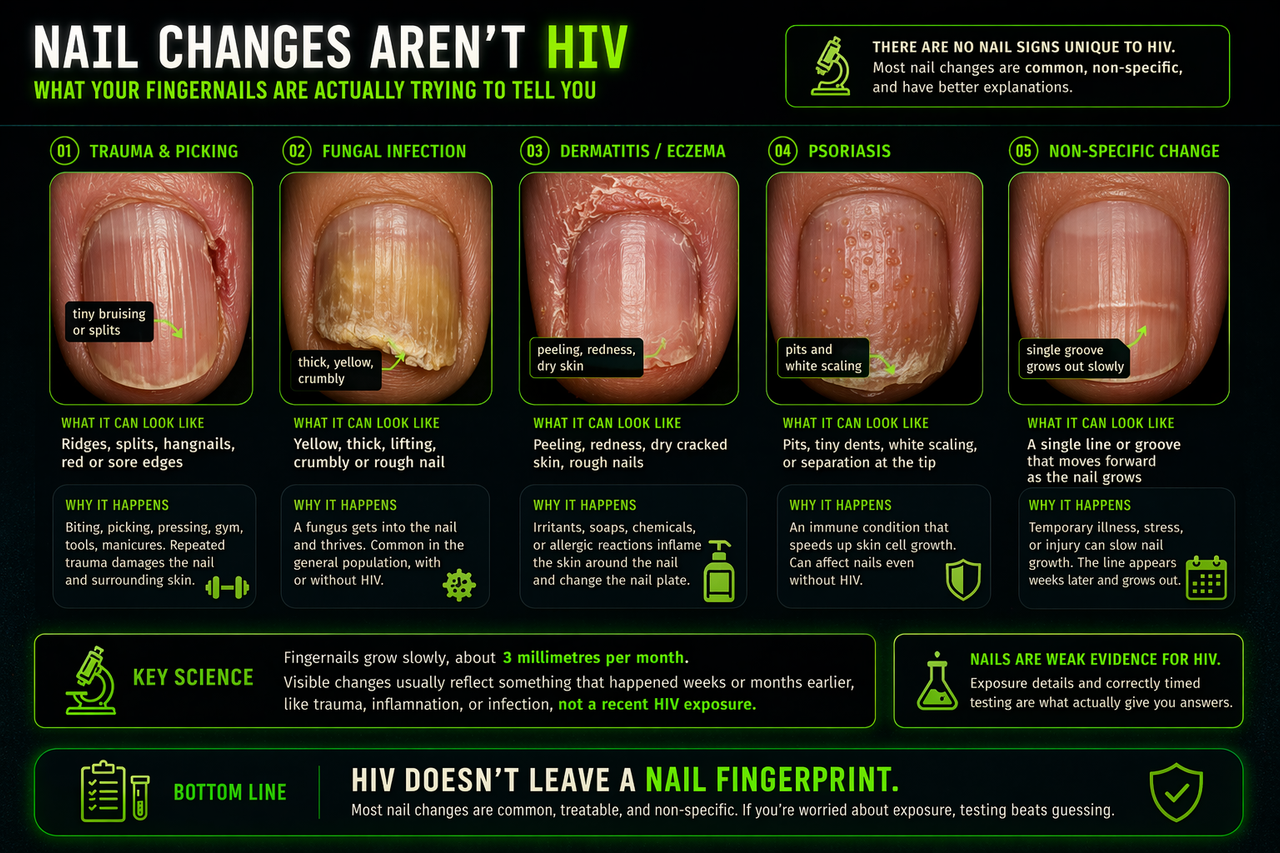
Common nail changes that are not specific to HIV
This graphic shows why fingernail changes usually have more common explanations such as trauma, fungus, dermatitis, psoriasis, or delayed non-specific growth changes. HIV does not leave a unique nail fingerprint.
What acute HIV usually looks like, and why nails are usually not part of that picture
In the first few weeks after HIV acquisition, if symptoms happen at all, they usually resemble a viral illness. Public health and HIV clinical sources describe things like fever, body rash, sore throat, swollen lymph nodes, fatigue, headaches, muscle or joint pains, and sometimes mouth ulcers or diarrhoea. That matters because it gives you a more reliable frame for what acute HIV does and does not usually look like.
Fingernails do not usually headline that early picture. There is no famous, pathognomonic “acute HIV fingernail sign” that doctors use to diagnose recent infection. So if someone notices ridges, splitting, colour change, peeling, brittle nails, or one damaged nail after a stressful sexual encounter, it is usually a bad idea to let anxiety turn that into a self-diagnosis.
The usual symptom lane
- Fever
- Body rash
- Sore throat
- Swollen glands
- Fatigue or malaise
- Headache, muscle aches, joint pain
A unique fingernail clue
A new nail ridge, mild brittleness, one discoloured nail, a hangnail, or a nail that looks “off” is not how acute HIV is typically recognised. Nails change slowly, and many nail problems come from trauma, moisture, picking, fungal infection, psoriasis, eczema, or normal wear and tear.
This does not mean HIV can never be associated with nail problems. It means nail changes are usually too non-specific to be useful as a standalone signal, especially in someone who is symptom-scanning because anxiety is running hurry-up offence.
Can HIV affect fingernails at all?
Yes, but usually indirectly and not in a way that lets you diagnose yourself from the mirror. Older dermatology literature and newer reviews describe a range of nail findings in people living with HIV, but the main takeaway is that there are no nail signs unique to HIV. Instead, clinicians think about broader categories.
Fungal nail infection
Onychomycosis, a fungal nail infection, is one of the better-known nail problems associated with immune suppression and has been reported more often in people with HIV, especially when disease is more advanced. It can cause thickening, yellow or white discolouration, crumbling, lifting, and involvement of multiple nails.
Medication-related changes
Some nail changes in HIV care have historically been linked to treatment, not the virus itself. Pigmented nails, especially darker streaking or diffuse darkening, have been described with zidovudine and other medication-related nail effects are also recognised in dermatology references.
Growth disruption
Severe illness, systemic stress, and immune dysfunction can affect nail growth. Beau’s lines, which are horizontal grooves that appear after nail growth temporarily slows, are non-specific and can happen after many illnesses, not just HIV.
Associated skin disease
Nail changes can also reflect skin conditions that may be more common or more severe in some people with HIV, such as psoriasis-like changes, chronic inflammation around the nail fold, or recurrent infections. Again, none of this is specific enough to diagnose HIV from the hand alone.
HIV can affect nails, but it usually does so through secondary mechanisms, not by creating a clean, instant, unmistakable nail fingerprint. That is why nail changes by themselves are weak tape. They do not tell you whether you have acute HIV.
Common fingernail problems that are much more likely than HIV
This is where most people get tripped up. Nails are small, visible, and slow to heal, which makes them perfect targets for anxious attention. But the everyday causes of fingernail changes are far more common than HIV.
Trauma and repetitive damage
- Nail biting or picking
- Pressing on the nail or cuticle
- Gym friction, tools, typing, gaming, manual work
- Manicures, gels, acetone, or harsh chemicals
Trauma can cause ridges, splits, tiny haemorrhages, white marks, tenderness, and uneven growth.
Fungal infection without HIV
Nail fungus is common in the general population. It does not require HIV. Thickening, yellowing, crumbly texture, nail lifting, and slow worsening over months fit fungal disease far better than acute HIV.
Eczema, psoriasis, dermatitis
Inflammatory skin conditions can change the nail plate and the surrounding skin. Pitting, roughness, inflammation around the nail fold, and dry cracked cuticles often point toward a dermatologic cause rather than an STI explanation.
Moisture and bacterial overgrowth
Constant wet work, picking at the cuticles, and damaged skin around the nails can lead to paronychia or greenish discolouration from secondary bacterial issues. Again, this is common and boring medicine, not a hidden HIV code.
If your nails suddenly seem brittle, ridged, weak, peeled, or “different”, anxiety will often try to connect that to the encounter you are worried about. But nails grow slowly. Many visible nail changes reflect events, inflammation, grooming habits, or trauma from weeks earlier. That lag alone makes them a poor tool for reading recent HIV risk.
Why fingernails are a brutal anxiety trigger
Fingernails are visible all day. You do not need a mirror to check them. That makes them perfect fuel for the “what if” loop. One tiny line, one area of peeling, one colour shift under bathroom lighting, and the mind starts building a case file.
Your brain starts overcalling weak evidence
- You keep checking the same nail multiple times a day.
- You compare it in different lighting.
- You search photos online until everything looks dangerous.
- You treat non-specific body noise as proof.
Because nails change slowly and visibly
Skin rashes come and go. Nails linger. That makes them feel more “serious”, even when the cause is minor. The problem is that visibility is not the same as diagnostic value.
The disciplined move is to separate symptom fear from actual HIV probability. Nail changes are weak evidence. Exposure type, condom use, partner likelihood, timing, and proper testing are strong evidence. That is how you stop anxiety from calling the plays.
What to do if you are worried
Audit the exposure, not the nail
Start with what actually happened. Was there vaginal or anal sex? Was a condom used? Was there a real transmission route? Nail changes do not decide HIV risk. Exposure does.
Use testing at the right time
HIV cannot be diagnosed from fingernails. If you had a meaningful exposure, follow an evidence-based testing timeline rather than symptom-scanning. That is the highest-standards play.
Treat the nail like a nail problem
If the nail is thickening, discolouring, painful, lifting, or the skin around it is inflamed, a GP, sexual health clinician, or dermatologist can assess it as a nail problem. They may think about fungus, trauma, eczema, psoriasis, paronychia, or other common causes first.
Break the checking loop
Pick one plan and run it. Stop repeated nail inspections. Stop comparing internet photos. Get the right test, at the right time, and let data carry the drive.
If you want a structured breakdown of your specific exposure, timing, and the real probability logic behind it, you can generate a private report based on your exact inputs.
Get My Confidential Risk ReportRed flags: when a fingernail problem needs medical review
- Severe pain, swelling, warmth, or pus around the nail.
- A black or brown streak that is new, widening, irregular, or also darkening the surrounding skin.
- Nail lifting or crumbling affecting multiple nails.
- Rapid change after a new medication.
- Associated fever or feeling very unwell.
These are not “HIV nail clues”. They are reasons to get the nail assessed properly.
Frequently Asked Questions
Acute HIV is usually discussed in terms of flu-like symptoms such as fever, rash, sore throat, fatigue, and swollen glands. Fingernail changes are not a classic or reliable early sign of recent HIV infection.
Yes. Nail problems can occur in people living with HIV, but they are generally non-specific and may relate to fungal infection, medication effects, growth disruption after illness, or associated skin disease. They do not provide a clean self-diagnosis.
Not by themselves. Fungal nail infection is common in the general population. It can be more frequent in immunocompromised people, including some people with HIV, but most nail fungus cases are not caused by HIV.
Dark nail pigmentation has been described in HIV settings, including medication-related changes, but pigmentation has many other causes too. A new or changing dark streak should be assessed medically because some pigmented nail changes need urgent review.
Worry should track the exposure, not the nail. Nail changes are weak evidence for HIV. If the encounter was low risk, the nail finding usually points elsewhere. If the encounter was higher risk, use proper testing rather than symptom interpretation.
No. HIV requires testing. Symptoms and nail changes overlap with many common, non-HIV conditions.
Sources & References
- HIV.gov, Symptoms of HIV: https://www.hiv.gov/hiv-basics/overview/about-hiv-and-aids/symptoms-of-hiv
- ClinicalInfo HIV.gov, Early (Acute and Recent) HIV Infection guideline: https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/special-populations-early-acute-recent-hiv-infection
- WHO, HIV and AIDS fact sheet: https://www.who.int/news-room/fact-sheets/detail/hiv-aids
- Daniel CR 3rd et al., The spectrum of nail disease in patients with human immunodeficiency virus infection: https://pubmed.ncbi.nlm.nih.gov/1619083/
- Cribier B et al., Nail changes in patients infected with human immunodeficiency virus: https://pubmed.ncbi.nlm.nih.gov/9801676/
- Flores-Bozo LR et al., Nail Changes in People Living with Human Immunodeficiency Virus: https://pmc.ncbi.nlm.nih.gov/articles/PMC9485993/
- DermNet, Fungal nail infections: https://dermnetnz.org/topics/fungal-nail-infections
- Merck Manual, Deformities, Dystrophies, and Discoloration of the Nails: https://www.msdmanuals.com/home/skin-disorders/nail-disorders/deformities-dystrophies-and-discoloration-of-the-nails
- DermNet, Cutaneous manifestations of human immunodeficiency virus: https://dermnetnz.org/cme/viral-infections/cutaneous-manifestations-of-human-immunodeficiency-virus
- DermNet, Drug-induced nail disease: https://dermnetnz.org/topics/drug-induced-nail-disease
This article is for education, not diagnosis or personal medical advice. If you think you had a meaningful HIV exposure, use a proper testing plan. If your nail is painful, infected, rapidly changing, or you feel systemically unwell, seek medical care.